Erwin Paul Campbell, Harris Jenine K, Smith Carson, Leep Carolyn J, Duggan Kathleen, Brownson Ross C
Department of Public Health, University of Tennessee, Knoxville, Tennessee (Dr Erwin); Prevention Research Center in St. Louis, Brown School, Washington University in St. Louis, St. Louis, Missouri (Drs Harris and Brownson); Division of Public Health Sciences and Alvin J. Siteman Cancer Center, Washington University School of Medicine, Washington University in St. Louis, St. Louis, Missouri (Ms Smith, Ms Duggan, and Dr Brownson); and National Association of County & City Health Officials, Washington, District of Columbia (Ms Leep).
J Public Health Manag Pract. 2014 Sep-Oct;20(5):472-80. doi: 10.1097/PHH.0000000000000027.
We assessed the use of administrative-evidence based practices (A-EBPs) among managers of programs in chronic diseases, environmental health, and infectious diseases from a sample of local health departments (LHDs) in the United States.
Program managers completed a survey consisting of 6 sections (biographical data, use of A-EBPs, diffusion attributes, use of resources, and barriers to, and competencies in, evidence-based public health), with a total of 66 questions.
The survey was sent electronically to 168 program managers in chronic diseases, 179 in environmental health, and 175 in infectious diseases, representing 228 LHDs. The survey had previously been completed by 517 LHD directors.
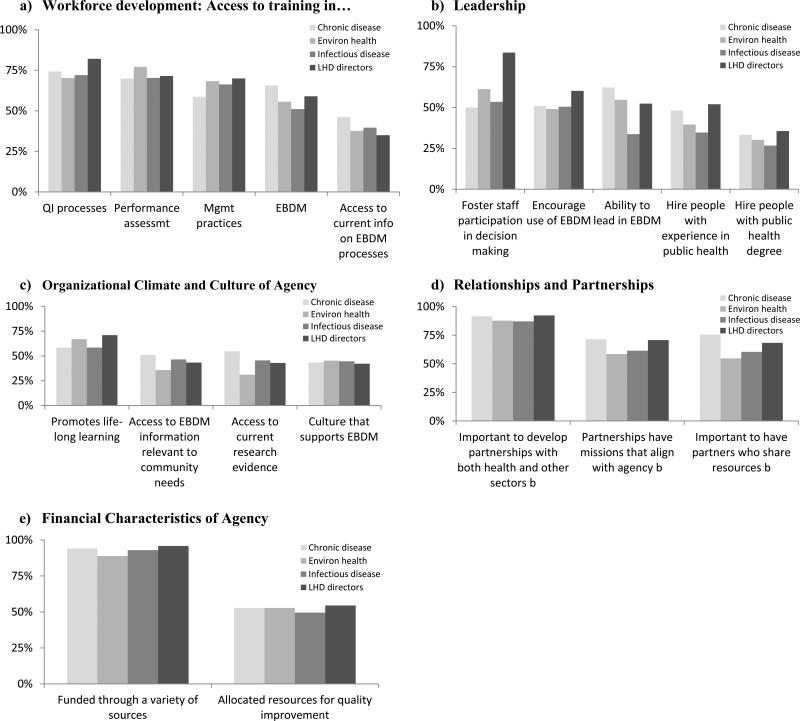
The use of A-EBPs was scored for 19 individual A-EBPs, across the 5 A-EBP domains, and for all domains combined. Individual characteristics were derived from the survey responses, with additional data on LHDs drawn from linked National Association of County & City Health Officials Profile survey data. Results for program managers were compared across the 3 types of programs and to responses from the previous survey of LHD directors. The scores were ordered and categorized into tertiles. Unconditional logistic regression models were used to calculate odds ratios and 95% confidence intervals, comparing individual and agency characteristics for those with the highest third of A-EBPs scores with those with the lowest third.
The 332 total responses from program managers represented 196 individual LHDs. Program managers differed (across the 3 programs, and compared with LHD directors) in demographic characteristics, education, and experience. The use of A-EBPs varied widely across specific practices and individuals, but the pattern of responses from directors and program managers was very similar for the majority of A-EBPs.
Understanding the differences in educational background, experience, organizational culture, and performance of A-EBPs between program managers and LHD directors is a necessary step to improving competencies in evidence-based public health.
我们对美国当地卫生部门(LHD)样本中慢性病、环境卫生和传染病项目的管理人员使用基于行政证据的实践(A-EBP)的情况进行了评估。
项目经理完成了一项由6个部分组成的调查(个人资料、A-EBP的使用、传播属性、资源利用以及循证公共卫生的障碍和能力),共有66个问题。
该调查以电子方式发送给168名慢性病项目经理、179名环境卫生项目经理和175名传染病项目经理,代表228个LHD。此前已有517名LHD主任完成了该调查。
对19种个体A-EBP在5个A-EBP领域以及所有领域的综合使用情况进行评分。个体特征来自调查回复,关于LHD的其他数据则取自美国县市卫生官员协会相关的概况调查数据。对3种类型项目的项目经理的结果进行比较,并与之前LHD主任调查的回复进行比较。分数按顺序排列并分为三分位数。使用无条件逻辑回归模型计算比值比和95%置信区间,比较A-EBP分数最高三分之一的人与最低三分之一的人的个体和机构特征。
项目经理的332份总回复代表了196个个体LHD。项目经理在人口统计学特征、教育程度和经验方面存在差异(在3个项目之间,以及与LHD主任相比)。A-EBP的使用在具体实践和个体之间差异很大,但对于大多数A-EBP来说,主任和项目经理的回复模式非常相似。
了解项目经理和LHD主任在教育背景、经验、组织文化以及A-EBP绩效方面的差异,是提高循证公共卫生能力的必要步骤。