Arnet Isabelle, Abraham Ivo, Messerli Markus, Hersberger Kurt E
Pharmaceutical Care Research Group, Department of Pharmaceutical Sciences, University of Basel, Klingelbergstr. 50, 4056, Basel, Switzerland,
Int J Clin Pharm. 2014 Feb;36(1):192-201. doi: 10.1007/s11096-013-9891-8. Epub 2013 Nov 29.
Several measures for calculating adherence to one medication from dispensing data records have been proposed, but the nomenclature is inconsistent and computations vary. The same measures, like the medication possession ratio (MPR), have been used for multiple medication regimens, and have tended to over- or under-estimate adherence rates.
To demonstrate the impact of varying elements in MPR to a single medication regimen; to define standards for the estimation of adherence to polypharmacy; to propose a new method for calculating adherence to polypharmacy; to face validate it.
Face validity of the proposed method.
Variations in the MPR formula were simulated. Standards for the estimation of adherence to polypharmacy were defined. A new method to calculate adherence to polypharmacy was established. Its face validity with three illustrative cases obtained from a pharmacy refill database was assessed.
Adherence rate to polypharmacy from refill data records.
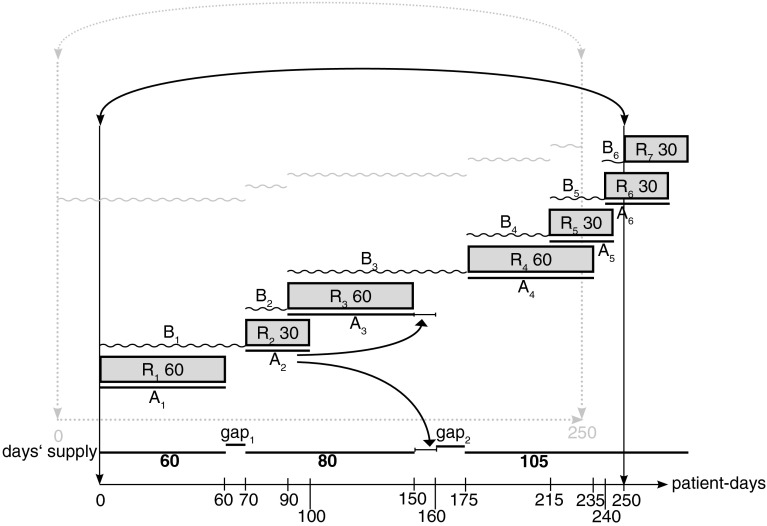
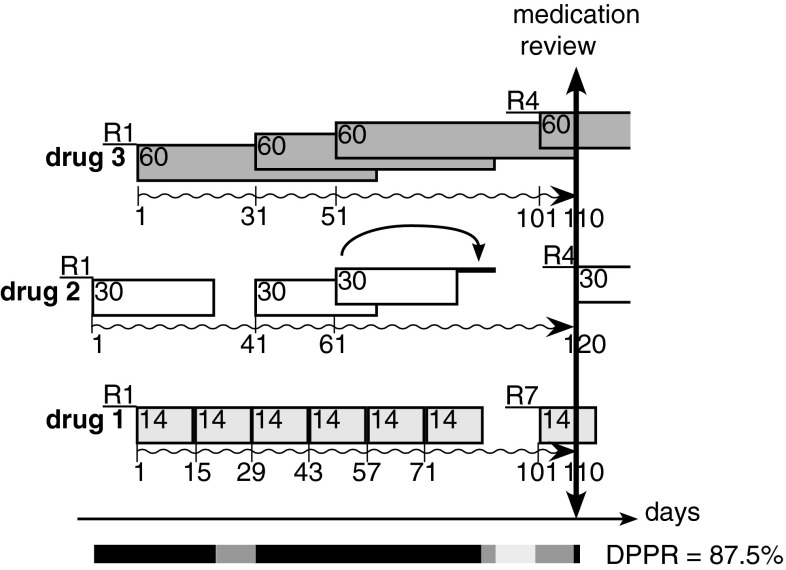
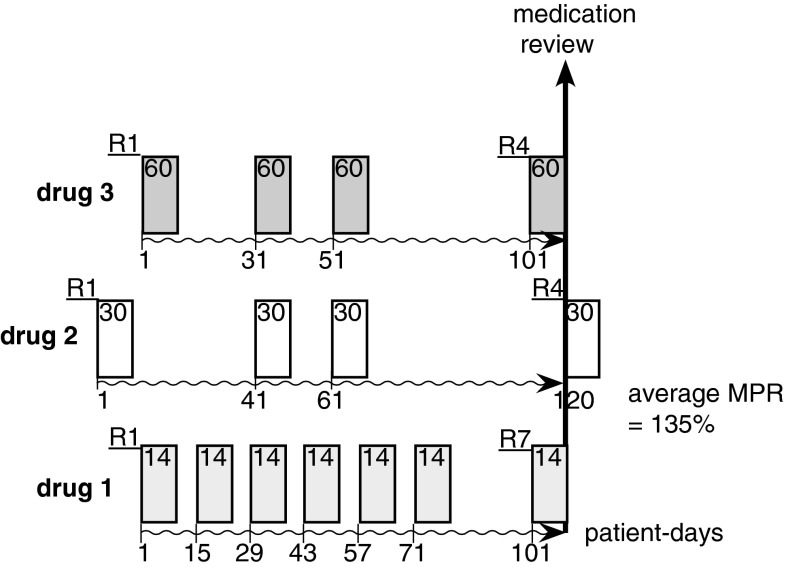
MPR to a single medication is operationalized in the numerator and denominator and is influenced by the parameters like observation period, medication gaps, overlap. For polypharmacy, an average MPR is commonly used, which is not accounting for the specificity of multiple medications, and hence overestimating adherence rate. We propose the daily polypharmacy possession ratio (DPPR) as an index of adherence to polypharmacy. It estimates the proportion of time a patient had medication available for use by considering the presence or absence of multiple medications on each day in the observation period. We calculated possession rates from refill histories over 31 months (January 1, 2011-July 31, 2013) for three illustrative patients. The average MPR estimates were 80 % for a patient with 6 medications/20 refill dates, 90 % for a patient with 4 medications/11 refill dates, and 89 % for a patient with 3 medications/17 refill dates. The corresponding DPPRs were 75, 88 and 99 %, indicating overestimations by 5 and 2 %, and underestimation by 10 %, respectively.
The DPPR accounts for the specificity of polypharmacy including number of medications, medication switching, duplication, overlapping. Research is needed to further confirm the validity of this new index.
已经提出了几种从配药数据记录计算单一药物依从性的方法,但术语不一致且计算方式各异。相同的方法,如药物持有率(MPR),已用于多种药物治疗方案,并且往往高估或低估依从率。
证明MPR中不同因素对单一药物治疗方案的影响;定义多药治疗依从性估计的标准;提出一种计算多药治疗依从性的新方法;进行表面效度验证。
所提方法的表面效度。
模拟MPR公式的变化。定义多药治疗依从性估计的标准。建立一种计算多药治疗依从性的新方法。评估其与从药房再填充数据库获得的三个示例病例的表面效度。
从再填充数据记录得出的多药治疗依从率。
单一药物的MPR在分子和分母中得以实施,并受观察期、用药间隔、重叠等参数影响。对于多药治疗,通常使用平均MPR,这未考虑多种药物的特殊性,因此高估了依从率。我们提出每日多药持有率(DPPR)作为多药治疗依从性的指标。它通过考虑观察期内每天是否存在多种药物来估计患者可使用药物的时间比例。我们计算了三个示例患者在31个月(2011年1月1日至2013年7月31日)期间再填充历史的持有率。对于一名服用6种药物/20次再填充的患者,平均MPR估计值为80%;对于一名服用4种药物/11次再填充的患者,为90%;对于一名服用3种药物/17次再填充的患者,为89%。相应的DPPR分别为75%、88%和99%,表明分别高估了5%和2%,低估了10%。
DPPR考虑了多药治疗的特殊性,包括药物数量、药物转换、重复、重叠。需要进一步研究以确认这一新指标的有效性。