Gharaibeh Almutez, Savage Howard I, Scherer Roberta W, Goldberg Morton F, Lindsley Kristina
Department of Special Surgery-Ophthalmology, Faculty of Medicine, The University of Jordan, P.O. Box 13046, Amman, Jordan.
Cochrane Database Syst Rev. 2013 Dec 3;12(12):CD005431. doi: 10.1002/14651858.CD005431.pub3.
Traumatic hyphema is the entry of blood into the anterior chamber (the space between the cornea and iris) subsequent to a blow or a projectile striking the eye. Hyphema uncommonly causes permanent loss of vision. Associated trauma (e.g. corneal staining, traumatic cataract, angle recession glaucoma, optic atrophy, etc.) may seriously affect vision. Such complications may lead to permanent impairment of vision. Patients with sickle cell trait/disease may be particularly susceptible to increases of elevated intraocular pressure. If rebleeding occurs, the rates and severity of complications increase.
To assess the effectiveness of various medical interventions in the management of traumatic hyphema.
We searched CENTRAL (which contains the Cochrane Eyes and Vision Group Trials Register) (The Cochrane Library 2013, Issue 8), Ovid MEDLINE, Ovid MEDLINE In-Process and Other Non-Indexed Citations, Ovid MEDLINE Daily, Ovid OLDMEDLINE (January 1946 to August 2013), EMBASE (January 1980 to August 2013), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrials.gov) and the WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en). We did not use any date or language restrictions in the electronic searches for trials. We last searched the electronic databases on 30 August 2013.
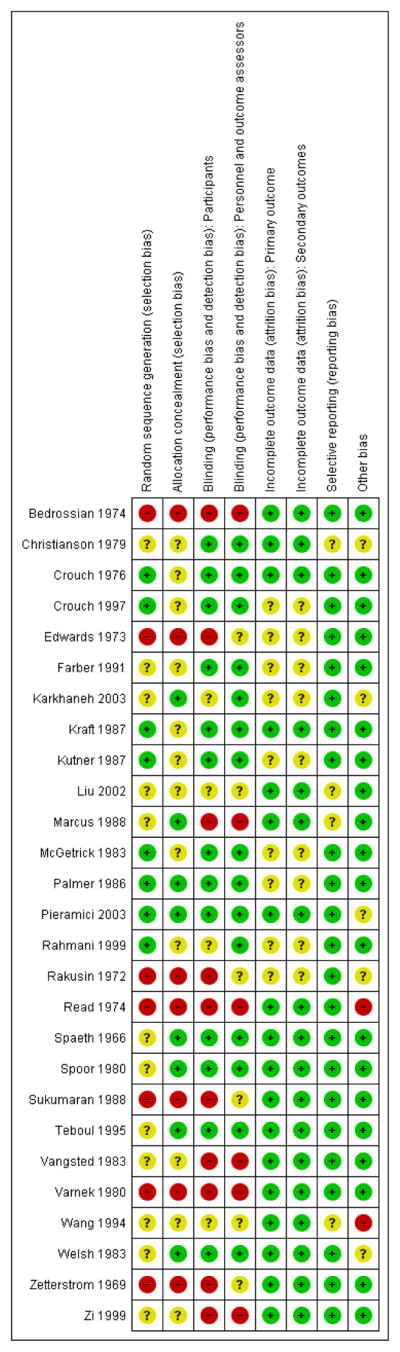
Two authors independently assessed the titles and abstracts of all reports identified by the electronic and manual searches. In this review, we included randomized and quasi-randomized trials that compared various medical interventions versus other medical interventions or control groups for the treatment of traumatic hyphema following closed globe trauma. We applied no restrictions regarding age, gender, severity of the closed globe trauma, or level of visual acuity at the time of enrolment.
Two authors independently extracted the data for the primary and secondary outcomes. We entered and analyzed data using Review Manager 5. We performed meta-analyses using a fixed-effect model and reported dichotomous outcomes as odds ratios and continuous outcomes as mean differences.
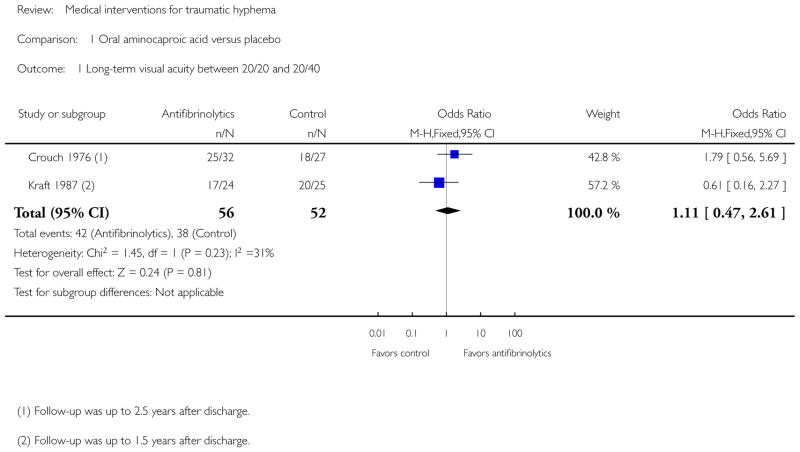
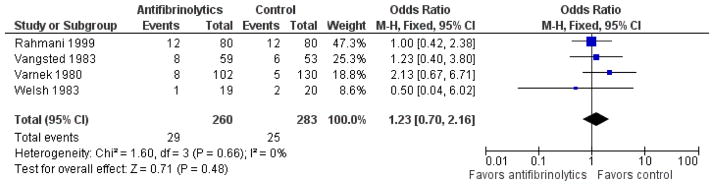
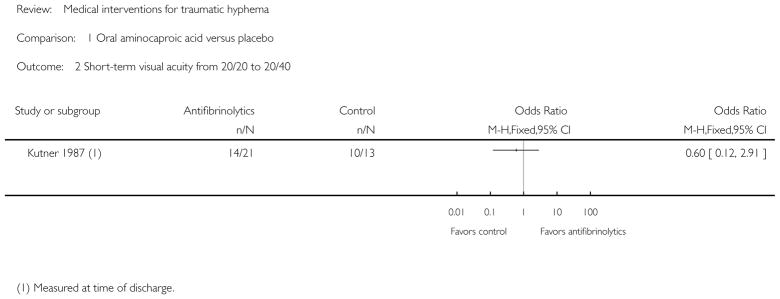
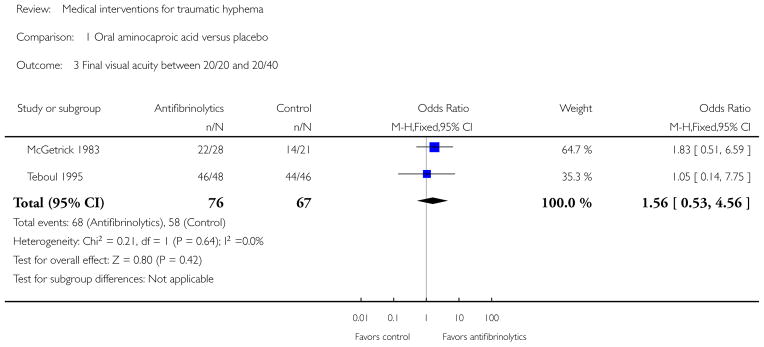
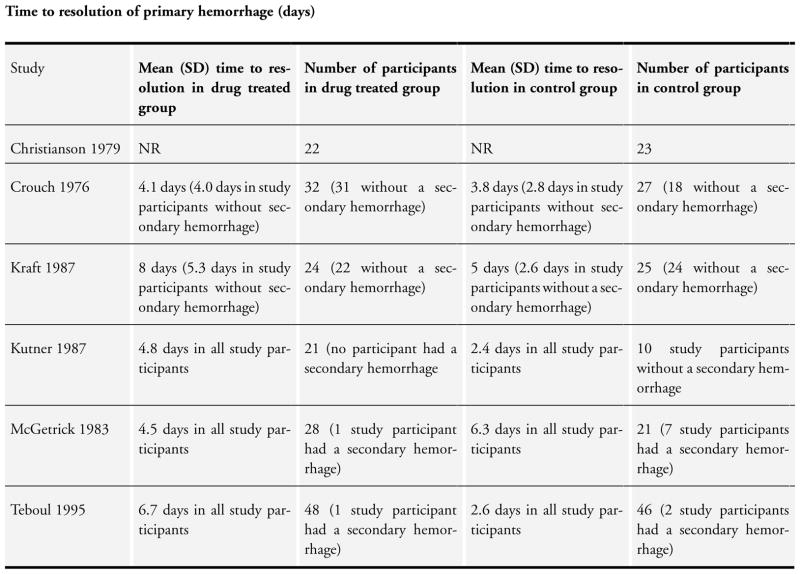
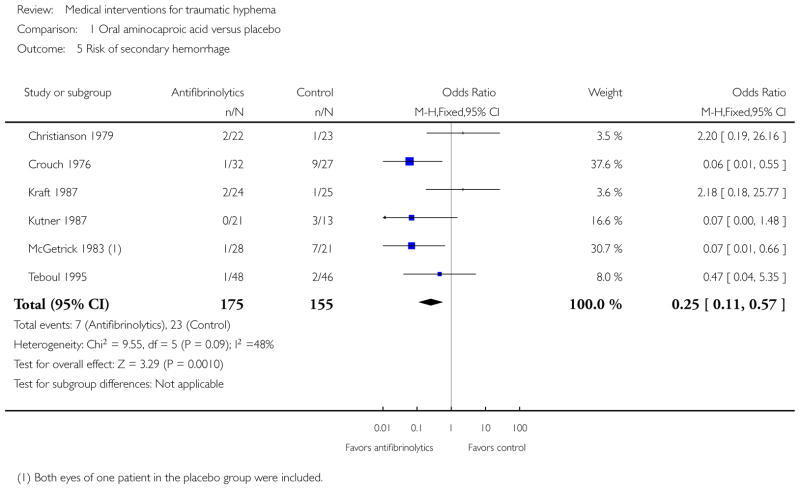
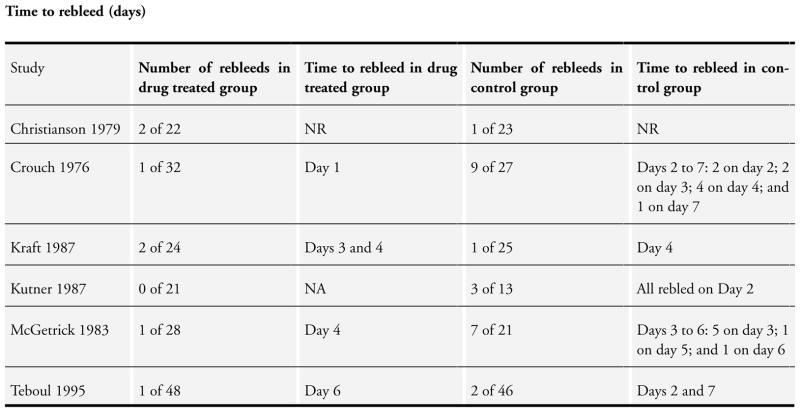
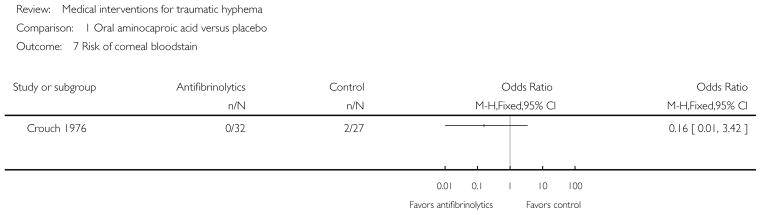
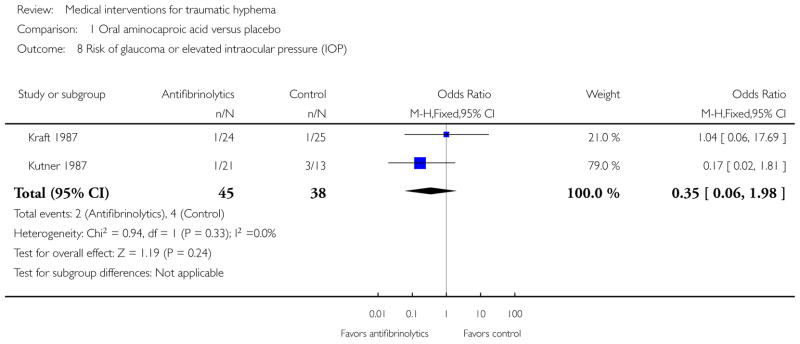
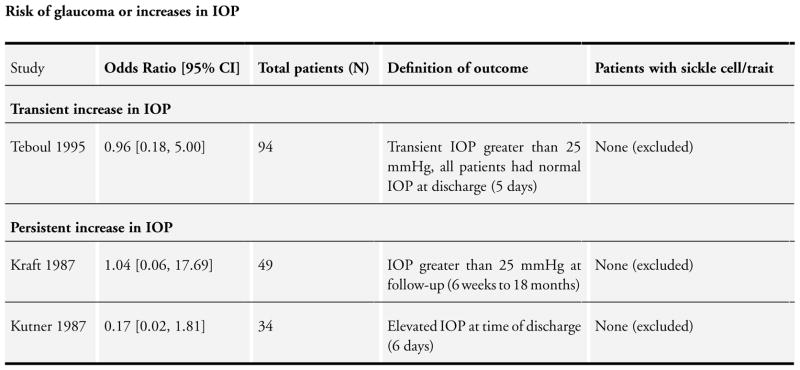
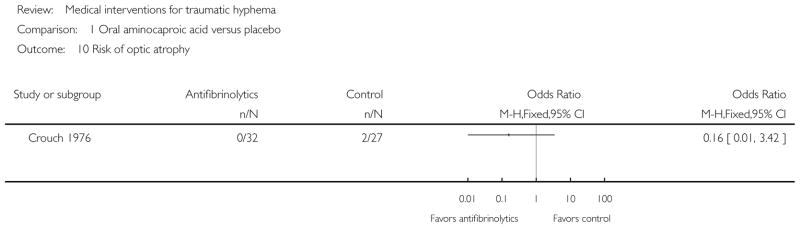
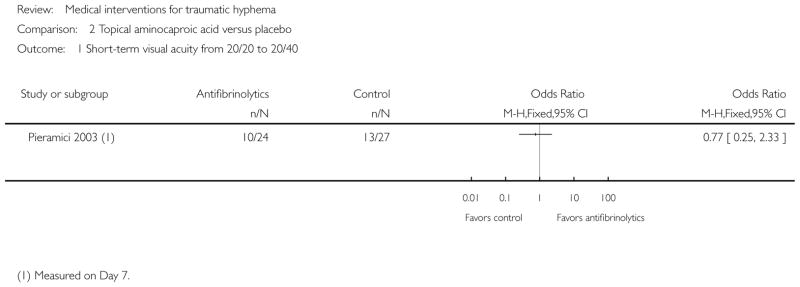
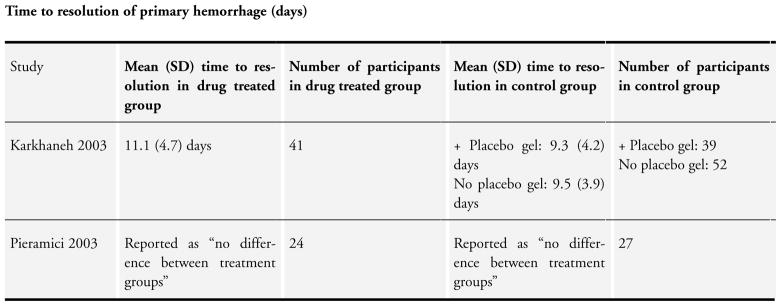
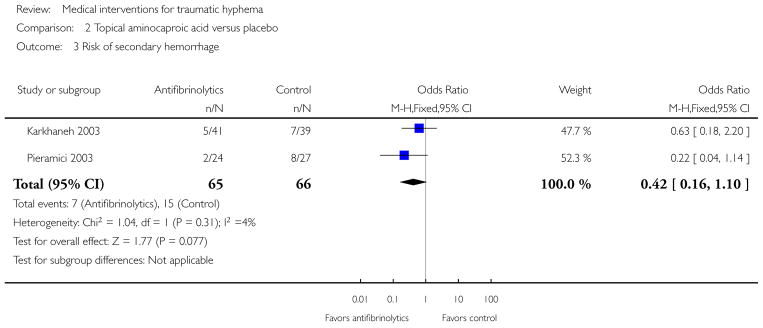
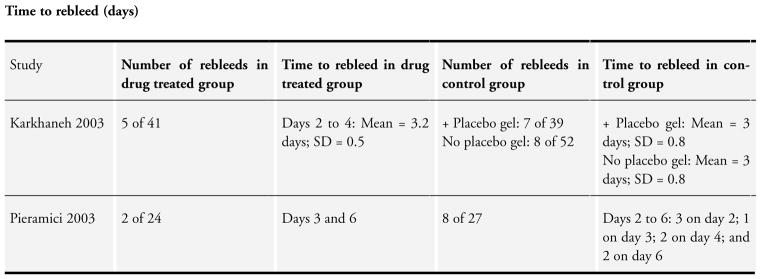
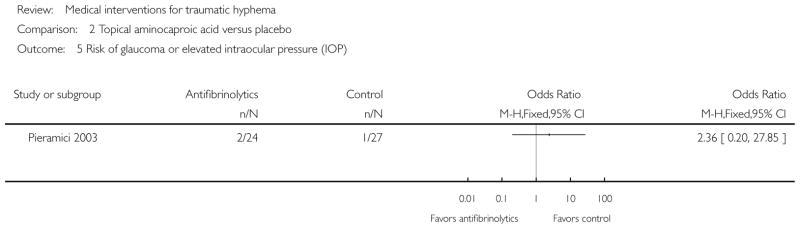
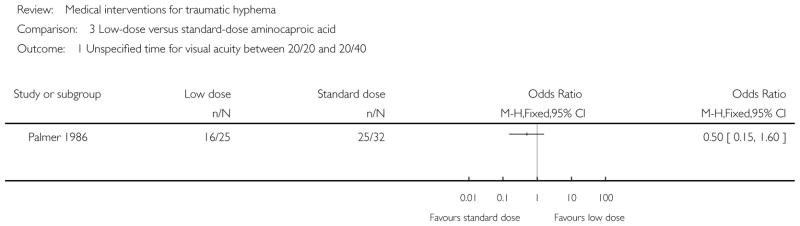
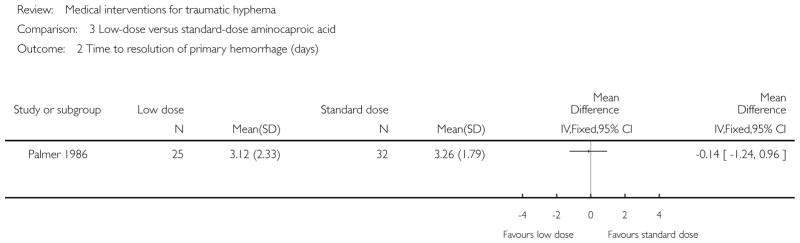
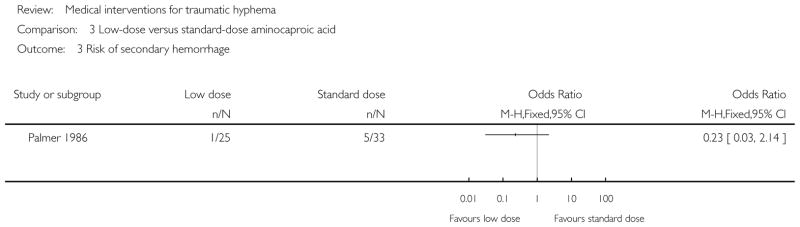
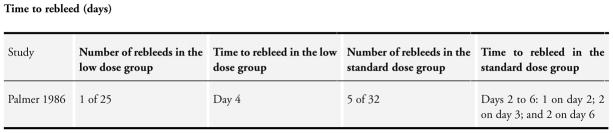
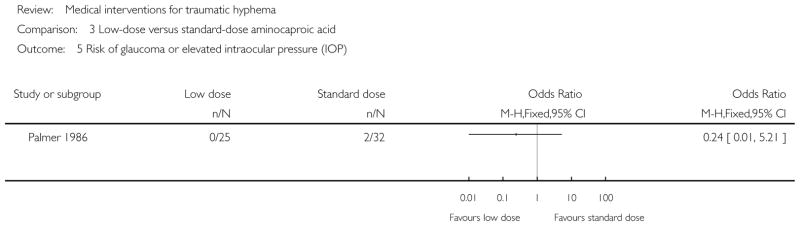
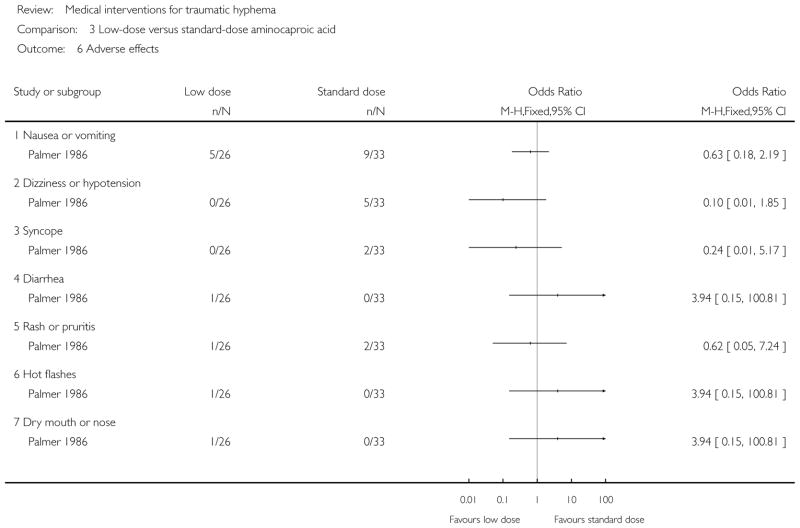
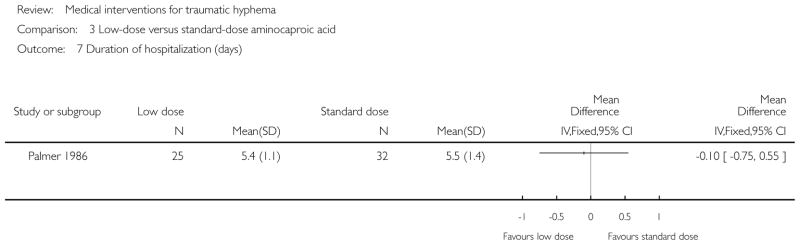
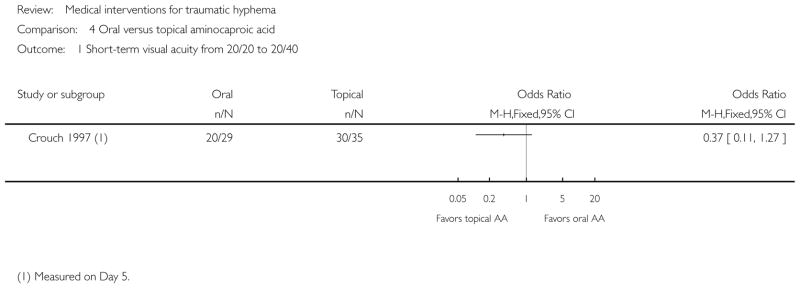
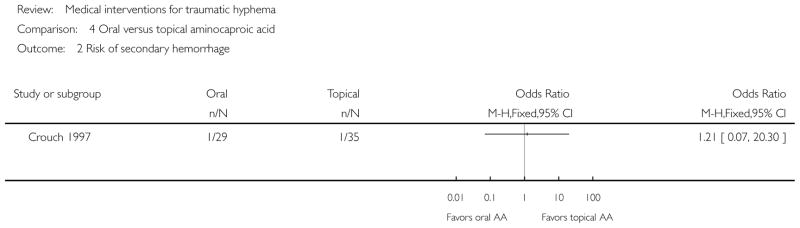
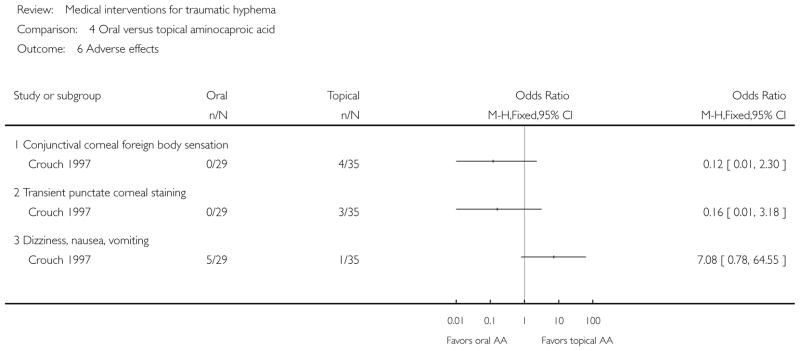
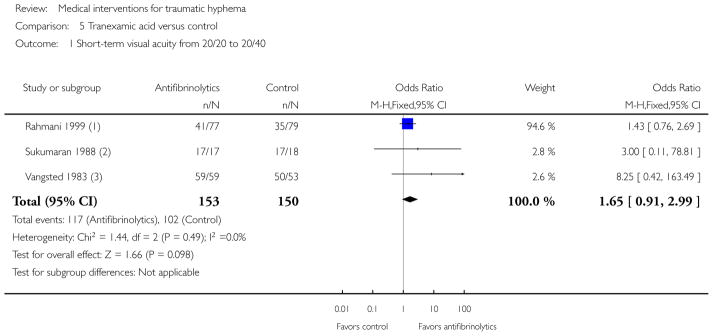
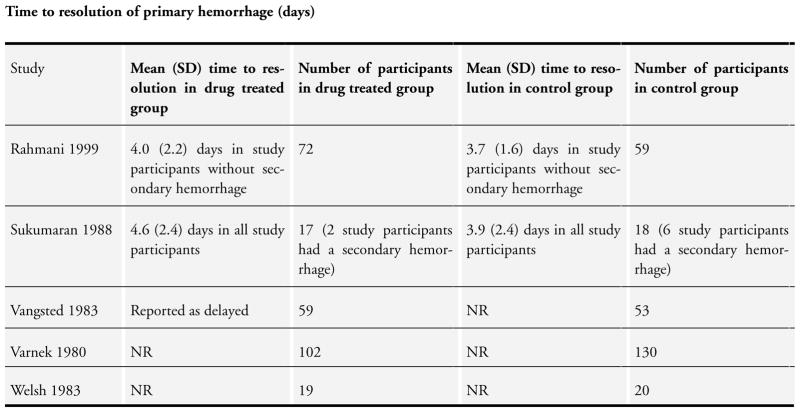
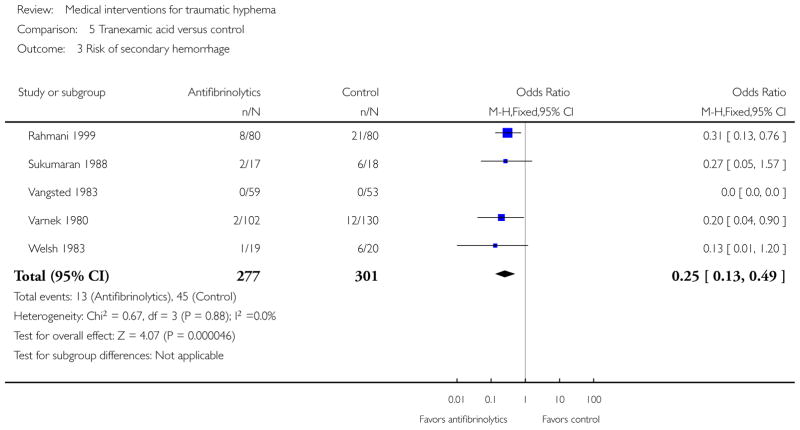
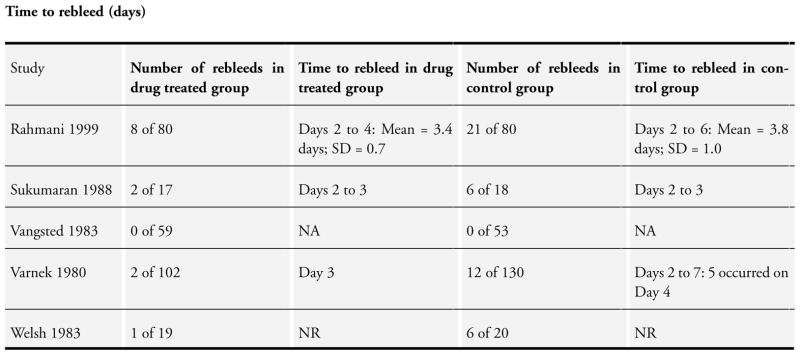
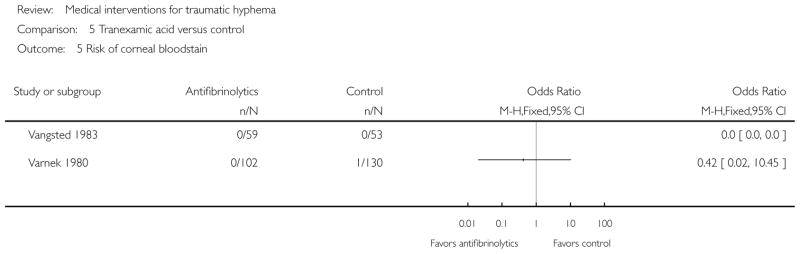
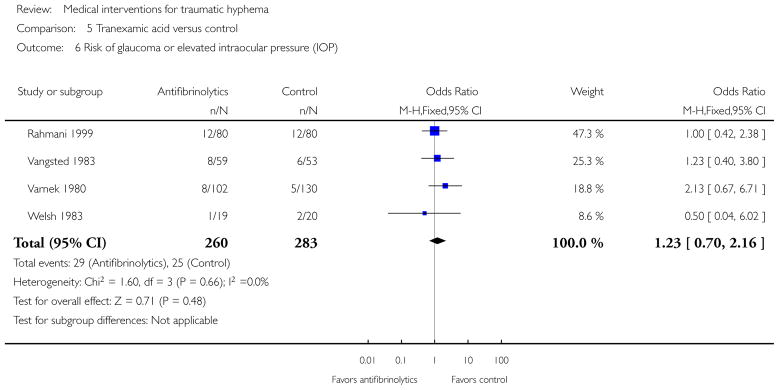
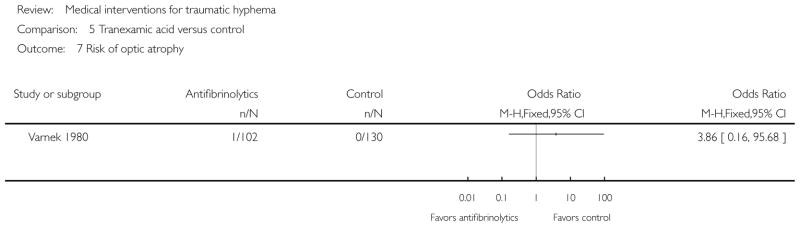
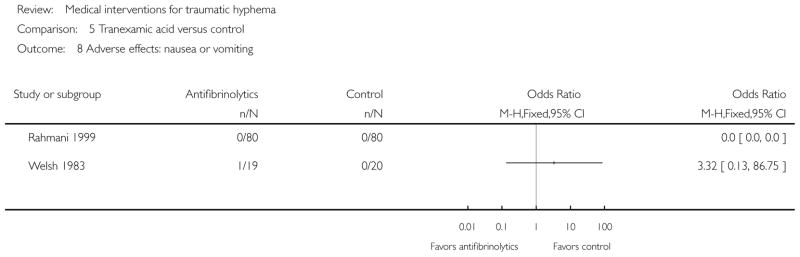
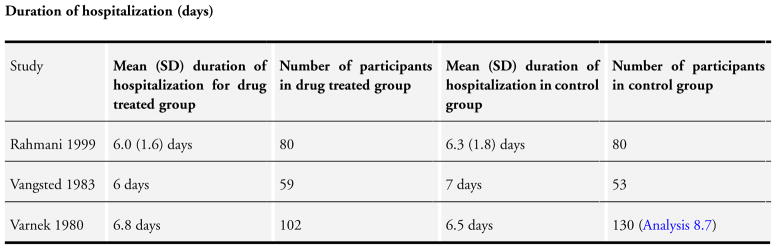
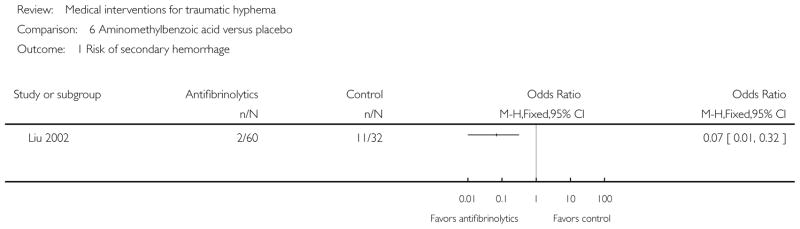
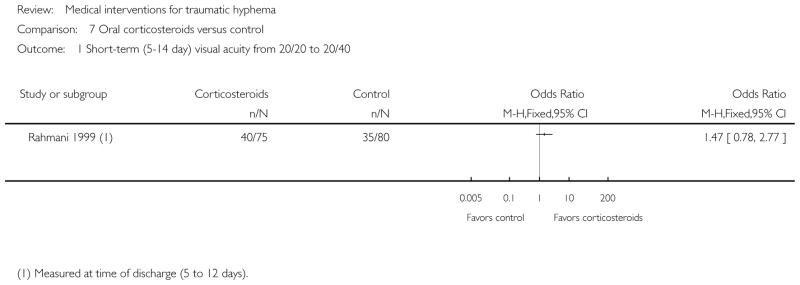
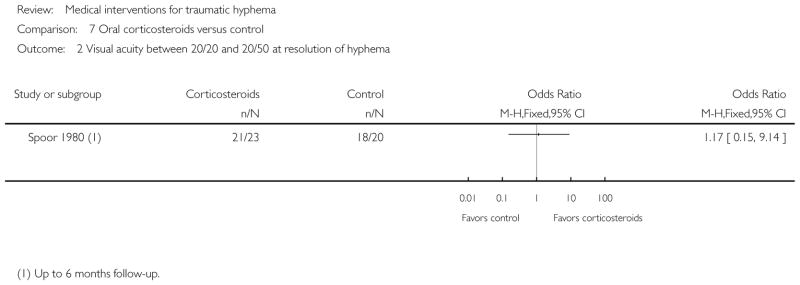
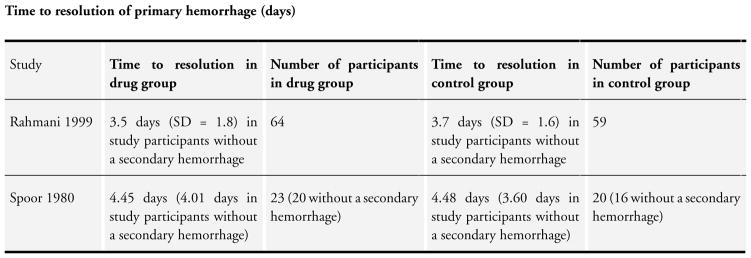
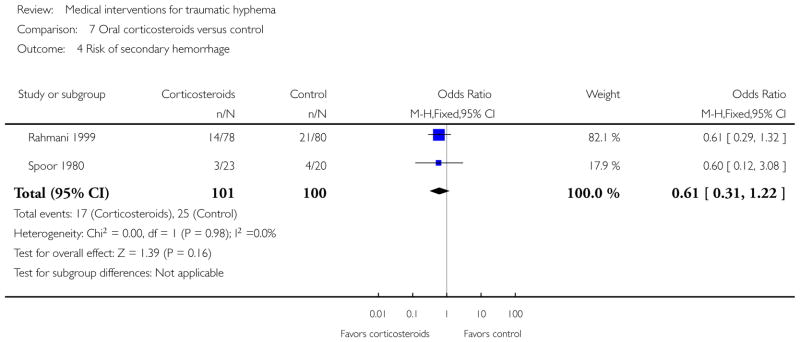
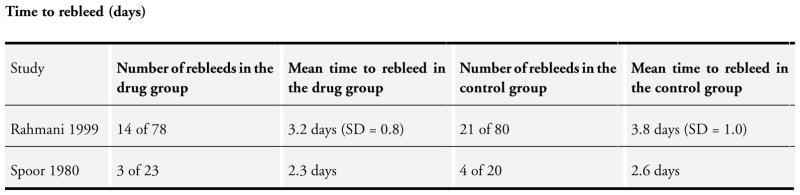
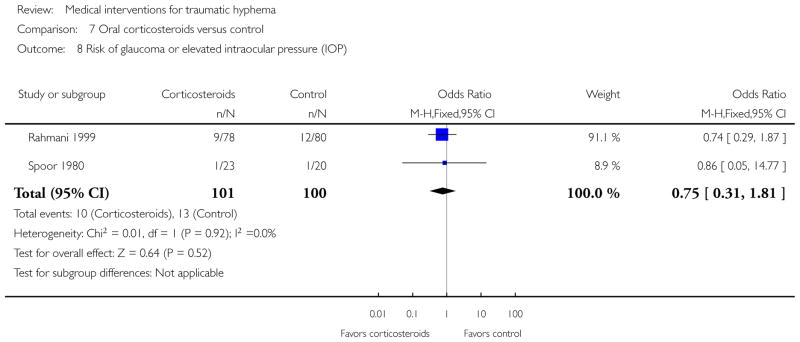
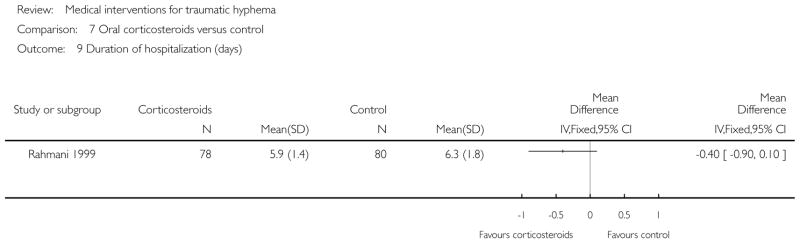
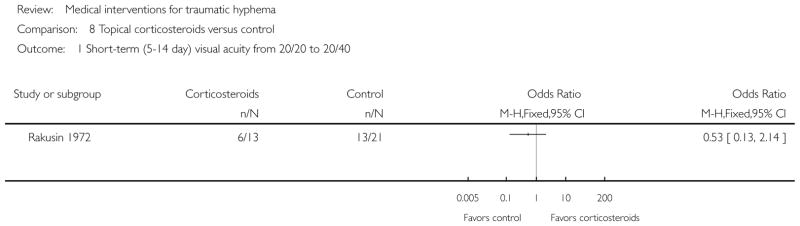
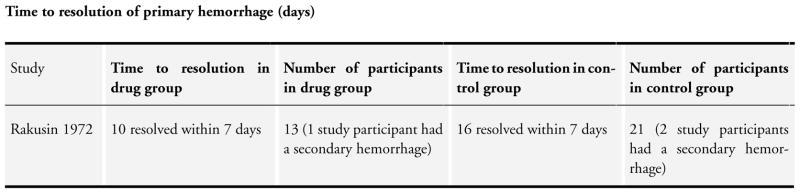
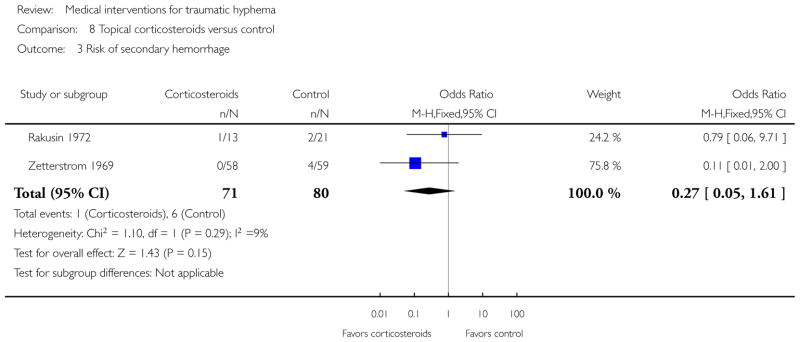
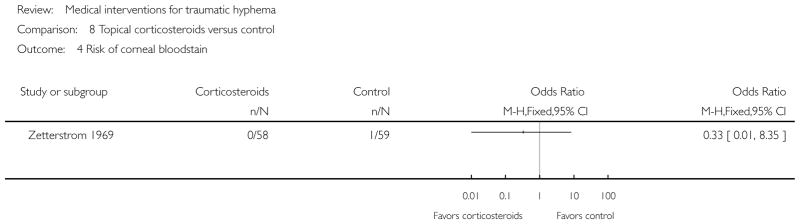
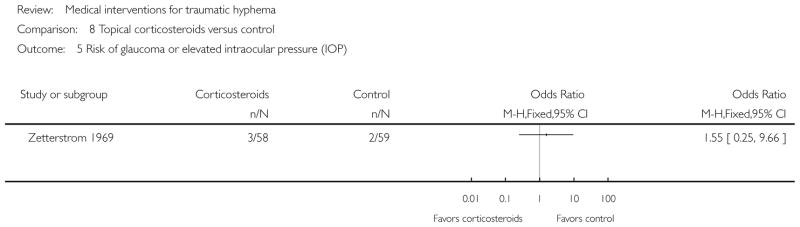
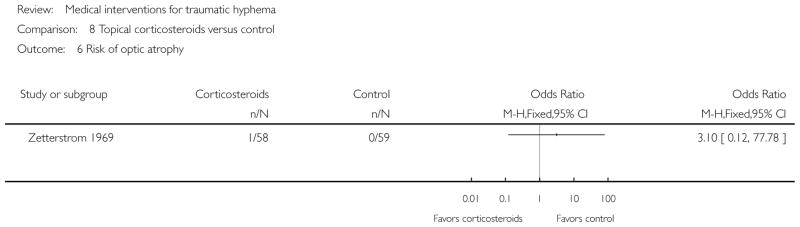
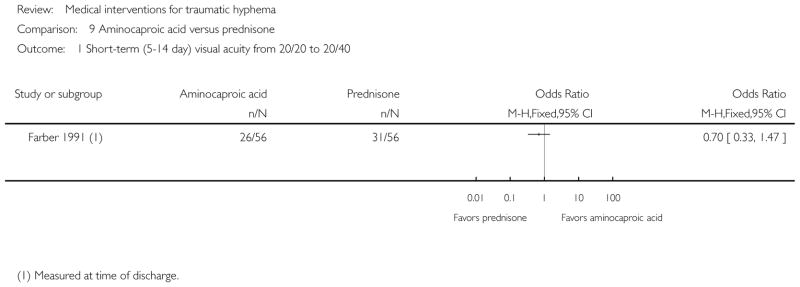
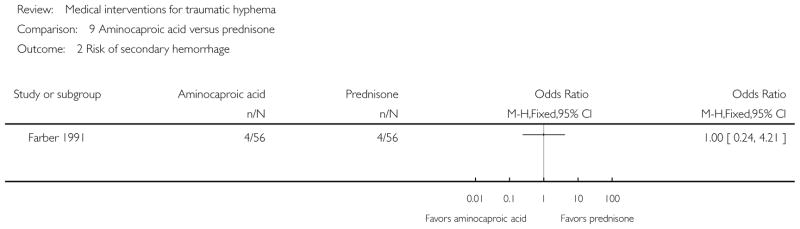
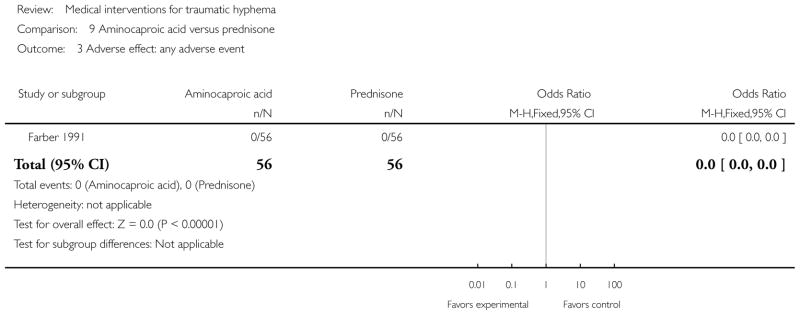
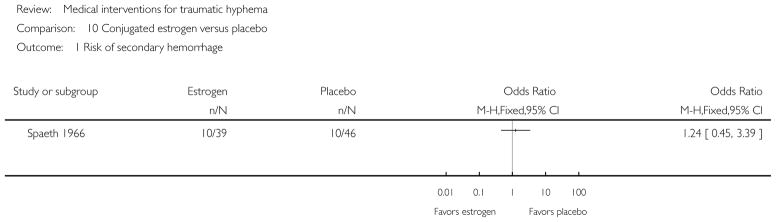
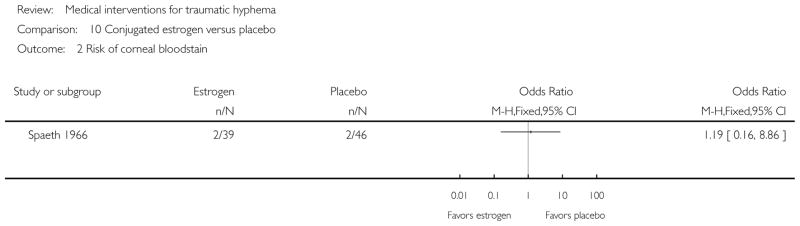
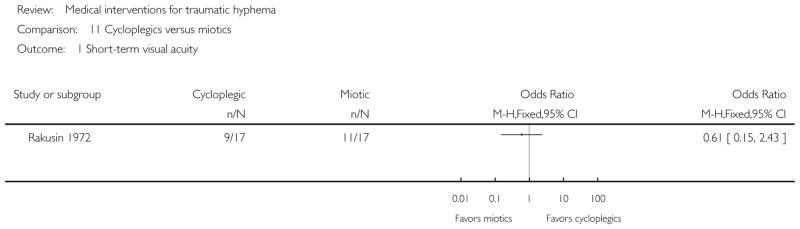
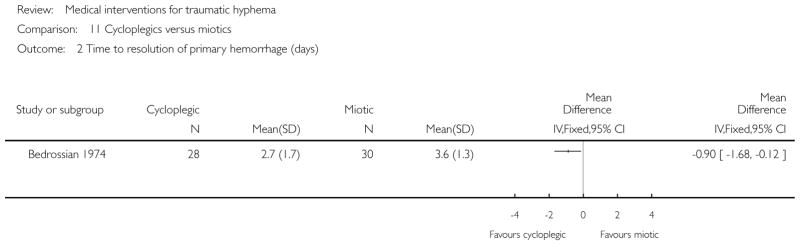
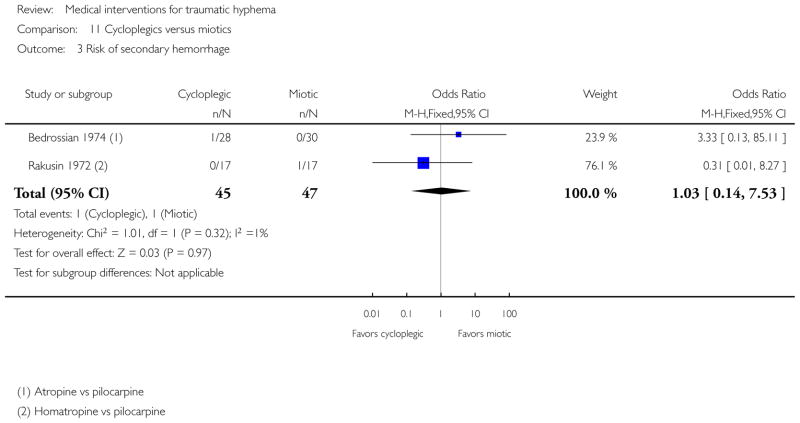
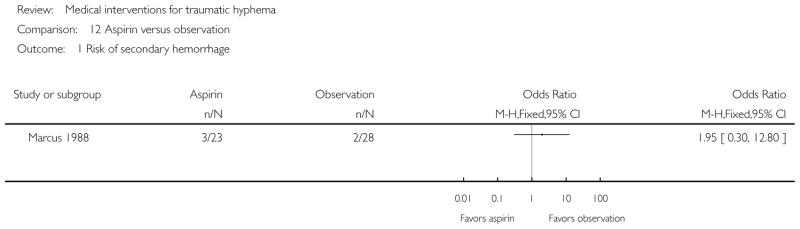
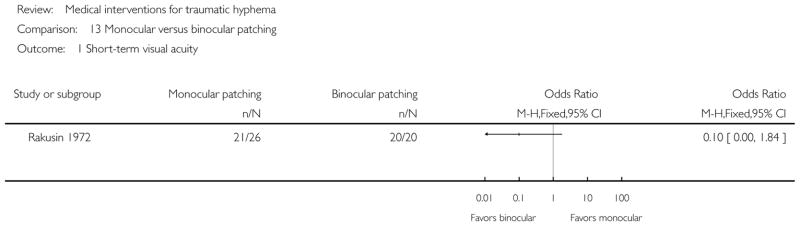
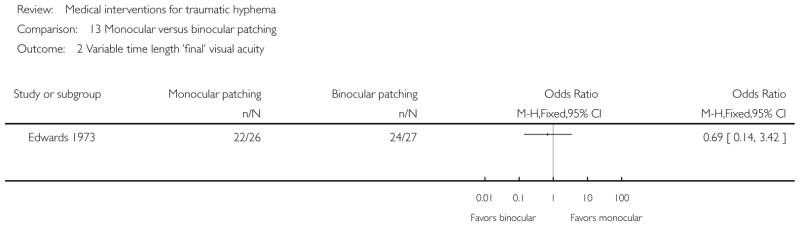
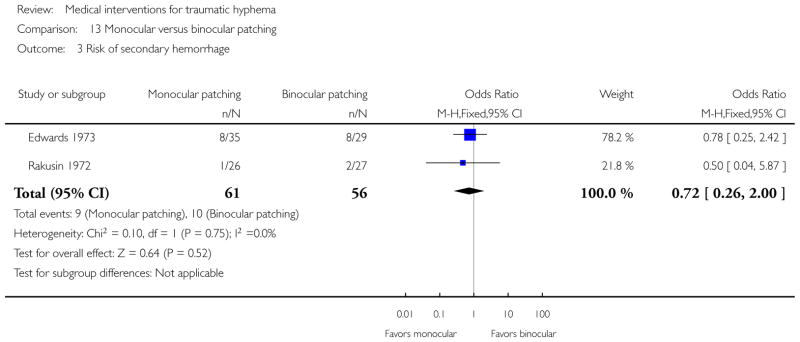
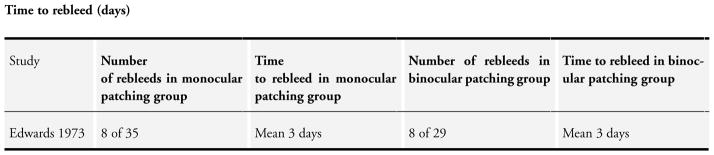
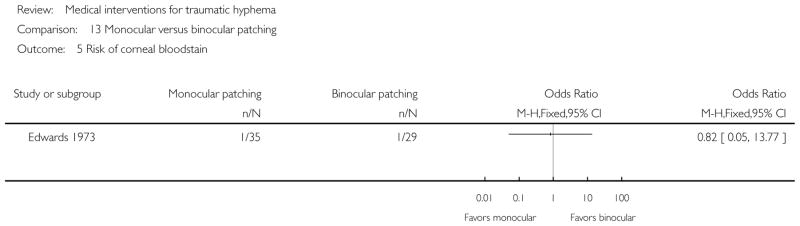
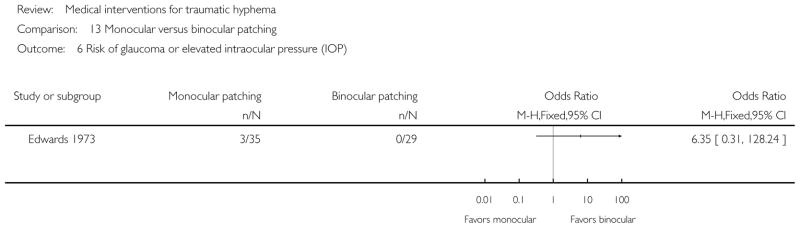
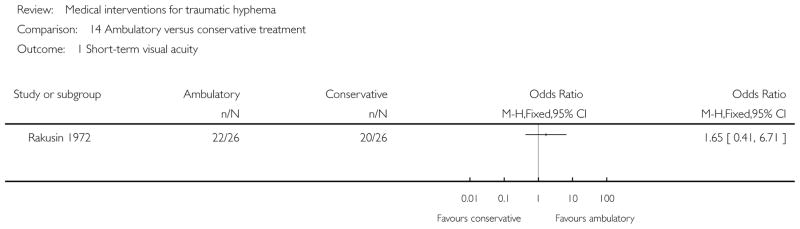
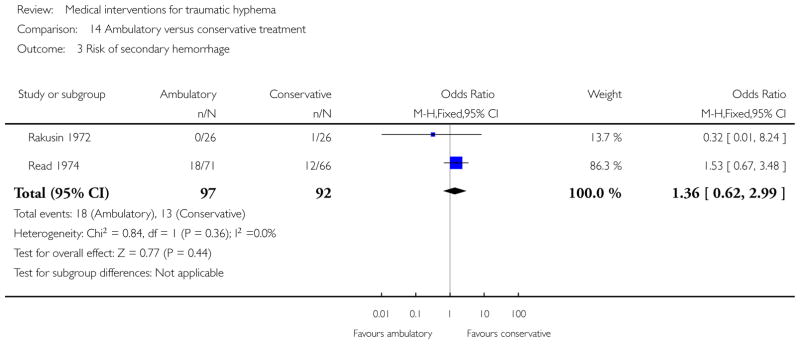
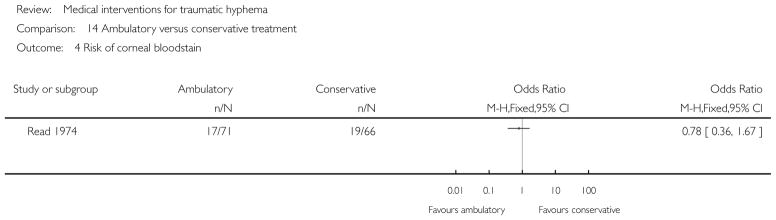
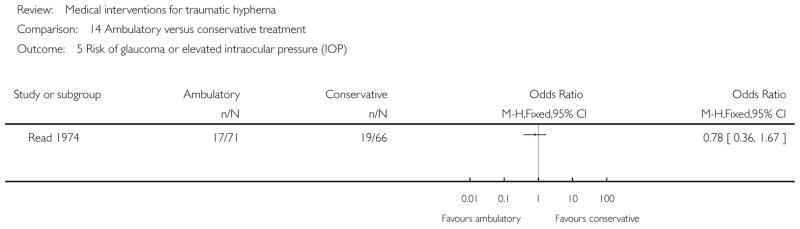
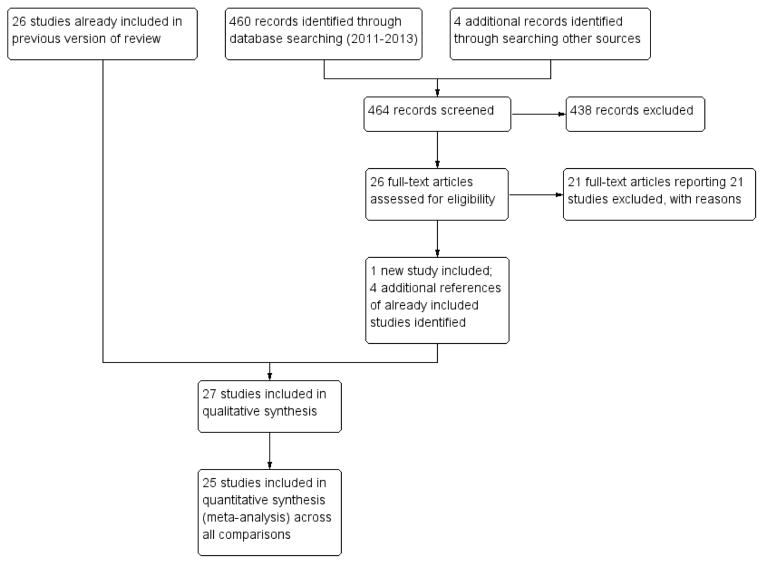
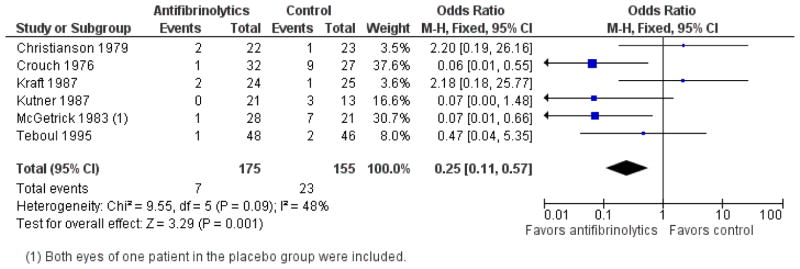
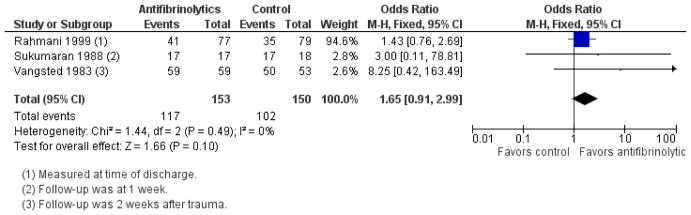
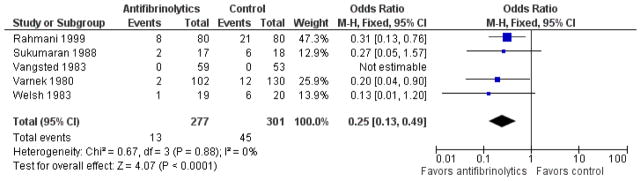
We included 20 randomized and seven quasi-randomized studies with 2643 participants in this review. Interventions included antifibrinolytic agents (oral and systemic aminocaproic acid, tranexamic acid, and aminomethylbenzoic acid), corticosteroids (systemic and topical), cycloplegics, miotics, aspirin, conjugated estrogens, traditional Chinese medicine, monocular versus bilateral patching, elevation of the head, and bed rest. No intervention had a significant effect on visual acuity whether measured at two weeks or less after the trauma or at longer time periods. The number of days for the primary hyphema to resolve appeared to be longer with the use of aminocaproic acid compared with no use, but was not altered by any other intervention.Systemic aminocaproic acid reduced the rate of recurrent hemorrhage (odds ratio (OR) 0.25, 95% confidence interval (CI) 0.11 to 0.57), but a sensitivity analysis omitting studies not using an intention-to-treat (ITT) analysis reduced the strength of the evidence (OR 0.41, 95% CI 0.16 to 1.09). We obtained similar results for topical aminocaproic acid (OR 0.42, 95% CI 0.16 to 1.10). We found tranexamic acid had a significant effect in reducing the rate of secondary hemorrhage (OR 0.25, 95% CI 0.13 to 0.49), as did aminomethylbenzoic acid as reported in one study (OR 0.07, 95% CI 0.01 to 0.32). The evidence to support an associated reduction in the risk of complications from secondary hemorrhage (i.e. corneal bloodstaining, peripheral anterior synechiae, elevated intraocular pressure, and development of optic atrophy) by antifibrinolytics was limited by the small number of these events. Use of aminocaproic acid was associated with increased nausea, vomiting, and other adverse events compared with placebo. We found no difference in the number of adverse events with the use of systemic versus topical aminocaproic acid or with standard versus lower drug dose. The available evidence on usage of corticosteroids, cycloplegics, or aspirin in traumatic hyphema was limited due to the small numbers of participants and events in the trials.We found no difference in effect between a single versus binocular patch or ambulation versus complete bed rest on the risk of secondary hemorrhage or time to rebleed.
AUTHORS' CONCLUSIONS: Traumatic hyphema in the absence of other intraocular injuries uncommonly leads to permanent loss of vision. Complications resulting from secondary hemorrhage could lead to permanent impairment of vision, especially in patients with sickle cell trait/disease. We found no evidence to show an effect on visual acuity by any of the interventions evaluated in this review. Although evidence was limited, it appears that patients with traumatic hyphema who receive aminocaproic acid or tranexamic acid are less likely to experience secondary hemorrhaging. However, hyphema in patients treated with aminocaproic acid take longer to clear.Other than the possible benefits of antifibrinolytic usage to reduce the rate of secondary hemorrhage, the decision to use corticosteroids, cycloplegics, or nondrug interventions (such as binocular patching, bed rest, or head elevation) should remain individualized because no solid scientific evidence supports a benefit. As these multiple interventions are rarely used in isolation, further research to assess the additive effect of these interventions might be of value.
外伤性前房积血是指眼球受到撞击或投射物打击后,血液进入前房(角膜和虹膜之间的间隙)。前房积血很少会导致永久性视力丧失。相关创伤(如角膜染色、外伤性白内障、房角后退性青光眼、视神经萎缩等)可能会严重影响视力。此类并发症可能导致永久性视力损害。镰状细胞性状/疾病患者可能特别容易出现眼压升高。如果发生再次出血,并发症的发生率和严重程度会增加。
评估各种医学干预措施治疗外伤性前房积血的有效性。
我们检索了Cochrane中心对照试验注册库(CENTRAL,其中包含Cochrane眼科和视力组试验注册库)(《Cochrane图书馆》2013年第8期)、Ovid MEDLINE、Ovid MEDLINE在研及其他非索引引文、Ovid MEDLINE每日更新、Ovid OLDMEDLINE(1946年1月至2013年8月)、EMBASE(1980年1月至2013年8月)、对照试验元注册库(mRCT)(www.controlled-trials.com)、ClinicalTrials.gov(www.clinicaltrials.gov)以及世界卫生组织国际临床试验注册平台(ICTRP)(www.who.int/ictrp/search/en)。在电子检索试验时,我们未设置任何日期或语言限制。我们最近一次检索电子数据库的时间为2013年8月30日。
两位作者独立评估了通过电子检索和手工检索确定的所有报告的标题和摘要。在本综述中,我们纳入了随机和半随机试验,这些试验比较了各种医学干预措施与其他医学干预措施或对照组在治疗闭合性眼球外伤后外伤性前房积血方面的效果。我们对纳入患者的年龄、性别、闭合性眼球外伤的严重程度或入组时的视力水平未作限制。
两位作者独立提取了主要和次要结局的数据。我们使用Review Manager 5录入和分析数据。我们采用固定效应模型进行Meta分析,并将二分法结局报告为比值比,将连续性结局报告为均值差。
本综述纳入了20项随机研究和7项半随机研究,共2643名参与者。干预措施包括抗纤维蛋白溶解剂(口服和全身应用氨基己酸、氨甲环酸和氨甲苯酸)、皮质类固醇(全身和局部应用)、睫状肌麻痹剂、缩瞳剂、阿司匹林、共轭雌激素、中药、单眼与双眼包扎、头部抬高和卧床休息。无论是在创伤后两周或更短时间测量,还是在更长时间段测量,没有任何干预措施对视力有显著影响。与未使用氨基己酸相比,使用氨基己酸时原发性前房积血消退的天数似乎更长,但其他任何干预措施均未改变这一情况。全身应用氨基己酸降低了再次出血的发生率(比值比(OR)0.25,95%置信区间(CI)0.11至0.57),但一项排除未采用意向性治疗(ITT)分析的研究的敏感性分析降低了证据强度(OR 0.41,95%CI 0.16至1.09)。局部应用氨基己酸也得到了类似结果(OR 0.42,95%CI 0.16至1.10)。我们发现氨甲环酸在降低继发性出血发生率方面有显著效果(OR 0.25,95%CI 0.13至0.49),一项研究报告氨甲苯酸也有此效果(OR 0.07,95%CI 0.01至0.32)。抗纤维蛋白溶解剂可降低继发性出血并发症(即角膜血染、周边前粘连、眼压升高和视神经萎缩的发生)风险的证据因这些事件数量较少而受限。与安慰剂相比,使用氨基己酸会增加恶心、呕吐及其他不良事件的发生。我们发现全身与局部应用氨基己酸或标准与低剂量药物使用时不良事件的数量没有差异。由于试验中参与者和事件数量较少,关于皮质类固醇、睫状肌麻痹剂或阿司匹林在治疗外伤性前房积血中的现有证据有限。我们发现单眼与双眼包扎或活动与完全卧床休息在继发性出血风险或再次出血时间方面没有效果差异。
在没有其他眼内损伤的情况下,外伤性前房积血很少导致永久性视力丧失。继发性出血引起的并发症可能导致永久性视力损害,尤其是镰状细胞性状/疾病患者。我们没有发现本综述中评估的任何干预措施对视力有影响的证据。虽然证据有限,但似乎接受氨基己酸或氨甲环酸治疗的外伤性前房积血患者发生继发性出血的可能性较小。然而,使用氨基己酸治疗的患者前房积血清除时间更长。除了抗纤维蛋白溶解剂可能有助于降低继发性出血发生率外,使用皮质类固醇、睫状肌麻痹剂或非药物干预措施(如双眼包扎、卧床休息或头部抬高)的决定应因人而异,因为没有确凿的科学证据支持其有益性。由于这些多种干预措施很少单独使用,进一步研究评估这些干预措施的叠加效果可能有价值。