Department of Rheumatology and Clinical Immunology, Medisch Spectrum Twente, Enschede, The Netherlands.
BMC Musculoskelet Disord. 2013 Dec 13;14:350. doi: 10.1186/1471-2474-14-350.
Where health economic studies are frequently performed using modelling, with input from randomized controlled trials and best guesses, we used real-life data to analyse the cost-effectiveness and cost-utility of a treatment strategy aiming to the target of remission compared to usual care in early rheumatoid arthritis (RA).
We used real-life data from comparable cohorts in the Dutch Rheumatoid Arthritis Monitoring (DREAM) registry: the DREAM remission induction cohort (treat-to-target, T2T) and the Nijmegen early RA inception cohort (usual care, UC). Both cohorts were followed prospectively using the DREAM registry methodology. All patients fulfilled the American College of Rheumatology criteria for RA and were included in the cohort at the time of diagnosis. The T2T cohort was treated according to a protocolised strategy aiming at remission (Disease Activity Score in 28 joints (DAS28) < 2.6). The UC cohort was treated without DAS28-guided treatment decisions. EuroQol-5D utility scores were estimated from the Health Assessment Questionnaire. A health care perspective was adopted and direct medical costs were collected. The incremental cost effectiveness ratio (ICER) per patient in remission and incremental cost utility ratio (ICUR) per quality-adjusted life year (QALY) gained were calculated over two and three years of follow-up.
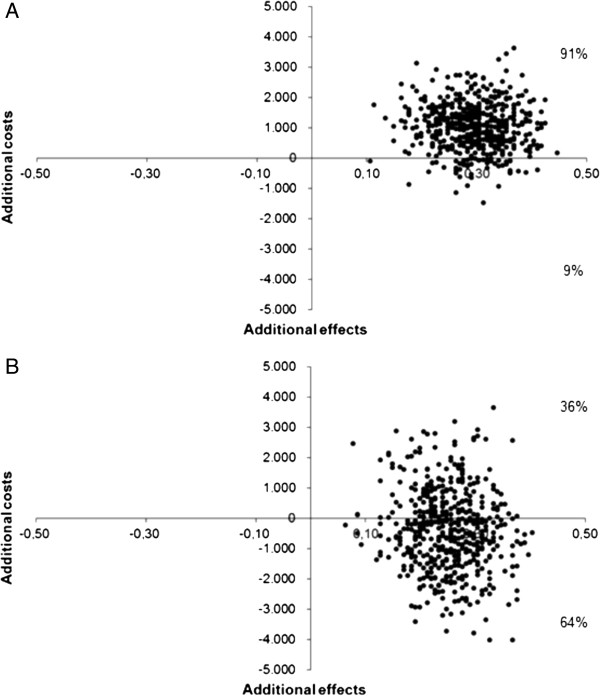
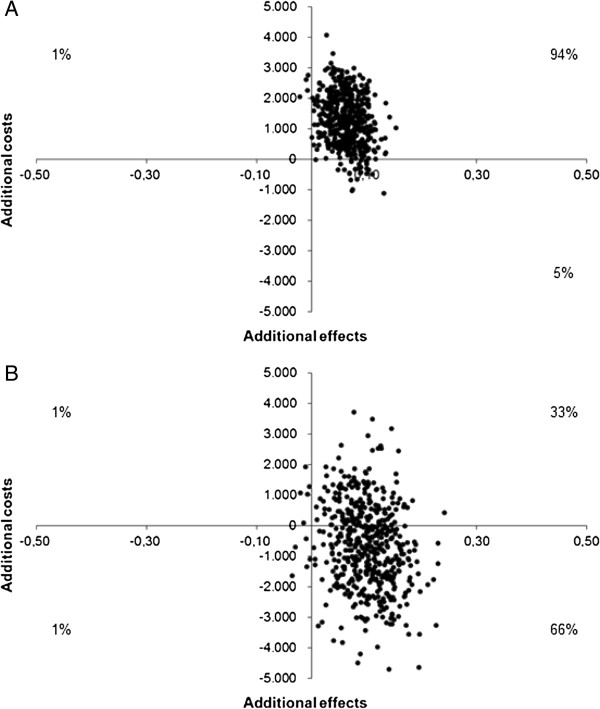
Two year data were available for 261 T2T patients and 213 UC patients; an extended follow-up of three years was available for 127 and 180 patients, respectively. T2T produced higher remission percentages and a larger gain in QALYs than UC. The ICER was € 3,591 per patient in remission after two years and T2T was dominant after three years. The ICUR was € 19,410 per QALY after two years and T2T was dominant after three years.
We can conclude that treating to the target of remission in early RA is cost-effective compared with UC. The data suggest that in the third year, T2T becomes cost-saving.
在进行健康经济研究时,通常会使用建模方法,并结合随机对照试验和最佳猜测结果,我们使用真实数据来分析旨在达到缓解目标的治疗策略与常规治疗相比在早期类风湿关节炎(RA)中的成本效益和成本效用。
我们使用荷兰类风湿关节炎监测(DREAM)注册中心中可比队列的真实数据:DREAM 缓解诱导队列(靶向治疗,T2T)和奈梅亨早期 RA 发病队列(常规治疗,UC)。两个队列都使用 DREAM 注册中心的方法进行前瞻性随访。所有患者均符合美国风湿病学会 RA 标准,并在诊断时纳入队列。T2T 队列按照旨在缓解(DAS28 < 2.6)的方案化策略进行治疗。UC 队列未进行 DAS28 指导的治疗决策。EuroQol-5D 效用评分从健康评估问卷中估算。采用医疗保健视角并收集直接医疗成本。在两年和三年的随访期间,计算每位缓解患者的增量成本效果比(ICER)和每获得一个质量调整生命年(QALY)的增量成本效用比(ICUR)。
两年的数据可用于 261 名 T2T 患者和 213 名 UC 患者;分别有 127 名和 180 名患者的随访时间延长至三年。T2T 产生的缓解百分比和 QALY 增益均高于 UC。两年后,T2T 每例缓解患者的 ICER 为 3591 欧元,三年后 T2T 占优势。两年后,T2T 每 QALY 的 ICUR 为 19410 欧元,三年后 T2T 占优势。
我们可以得出结论,与 UC 相比,在早期 RA 中达到缓解目标的治疗具有成本效益。数据表明,在第三年,T2T 具有成本节约效益。