Mahil S K, Wilson N, Dand N, Reynolds N J, Griffiths C E M, Emsley R, Marsden A, Evans I, Warren R B, Stocken D, Barker J N, Burden A D, Smith C H
St John's Institute of Dermatology, Guy's and St Thomas' NHS Foundation Trust, London, U.K.
Institute of Health and Society, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, U.K.
Br J Dermatol. 2020 May;182(5):1158-1166. doi: 10.1111/bjd.18333. Epub 2019 Sep 10.
The 'treat to target' paradigm improves outcomes and reduces costs in chronic disease management but is not yet established in psoriasis.
To identify treatment targets in psoriasis using two common measures of disease activity: Psoriasis Area and Severity Index (PASI) and Physician's Global Assessment (PGA).
Data from a multicentre longitudinal U.K. cohort of patients with psoriasis receiving systemic or biologic therapies (British Association of Dermatologists Biologics and Immunomodulators Register, BADBIR) were used to identify absolute PASI thresholds for 90% (PASI 90) and 75% (PASI 75) improvements in baseline disease activity, using receiver operating characteristic curves. The relationship between PGA (clear, almost clear, mild, moderate, moderate-severe, severe) and PASI (range 0-72) was described, and the concordance between absolute and relative definitions of response was determined. The same approach was used to establish treatment response and eligibility definitions based on PGA.
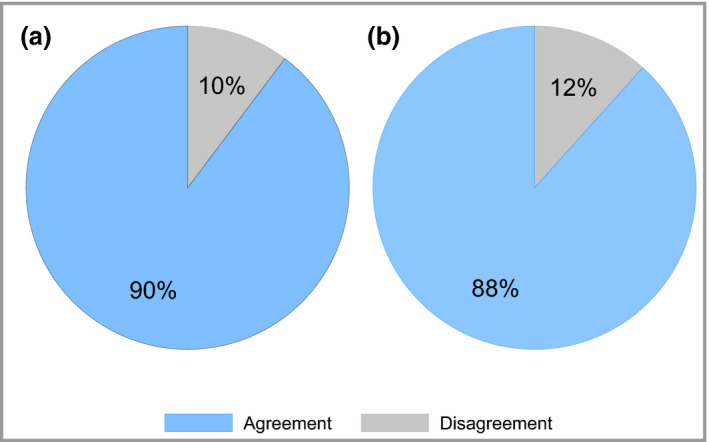
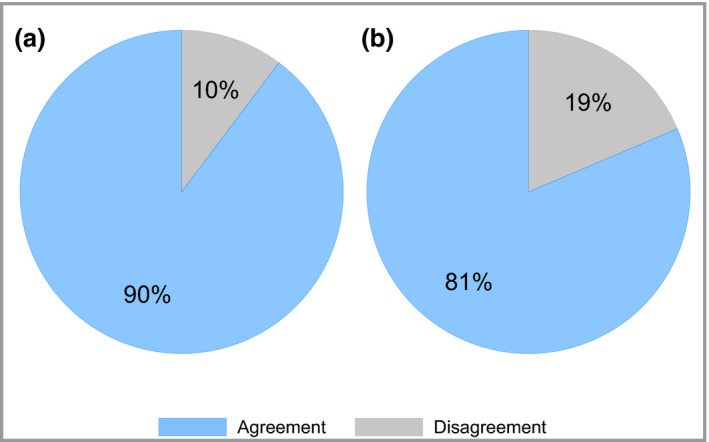
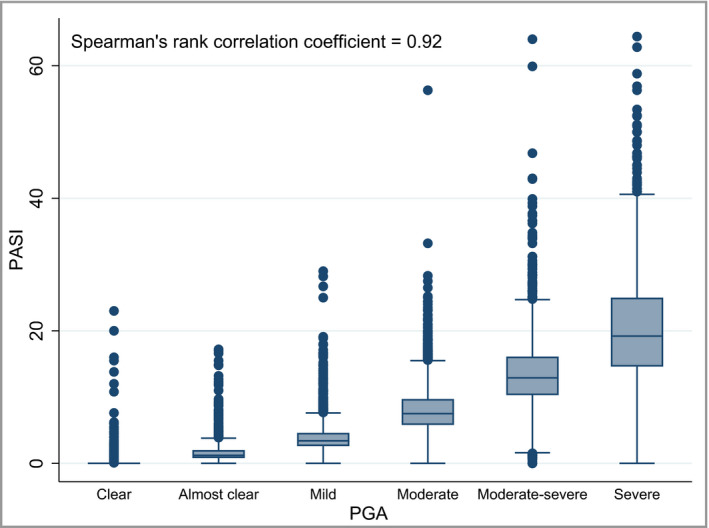
Data from 13 422 patients were available (58% male, 91% white ethnicity, mean age 44·9 years), including over 23 000 longitudinal PASI and PGA scores. An absolute PASI ≤ 2 was concordant with PASI 90 and an absolute PASI ≤ 4 was concordant with PASI 75 in 90% and 88% of cases, respectively. These findings were robust to subgroups of timing of assessment, baseline disease severity and treatment modality. PASI and PGA were strongly correlated (Spearman's rank correlation coefficient 0·92). The median PASI increased from 0 (interquartile range 0-0, range 0-23) to 19 (interquartile range 15-25, range 0-64) for PGA clear to severe, respectively. PGA clear/almost clear was concordant with PASI ≤ 2 in 90% of cases, and PGA moderate-severe severe was concordant with the National Institute for Health and Care Excellence PASI eligibility criteria for biologics in 81% of cases.
An absolute PASI ≤ 2 and PGA clear/almost clear represent relevant disease end points to inform treat-to-target management strategies in psoriasis. What's already known about this topic? The most commonly used relative disease activity measure in psoriasis is ≥ 90% improvement in Psoriasis Area and Severity Index (PASI 90); however, it has several limitations including dependency on a baseline severity assessment. Defining an absolute target disease activity end point in psoriasis has the potential to improve patient outcomes and reduce costs, as demonstrated by treat-to-target approaches in other chronic diseases such as hypertension and diabetes. The Physician's Global Assessment (PGA) is a popular alternative measure of psoriasis severity in daily practice; however, its utility has not been formally assessed with respect to PASI. What does this study add? An absolute PASI ≤ 2 corresponds with PASI 90 response and is a relevant disease end point for treat-to-target approaches in psoriasis. There is a strong correlation between PASI and PGA. PGA moderate-severe/severe may serve as an alternative eligibility criterion for biologics to PASI-based definitions, and PGA clear/almost clear is an appropriate alternative absolute treatment end point. What are the clinical implications of this work? Absolute PASI ≤ 2 and PGA clear/almost clear represent relevant disease end points to inform treat-to-target management strategies in psoriasis.
“治疗达标”模式可改善慢性病管理的结局并降低成本,但在银屑病中尚未确立。
使用两种常见的疾病活动度测量方法,即银屑病面积和严重程度指数(PASI)及医生整体评估(PGA),来确定银屑病的治疗靶点。
利用来自英国一个多中心纵向队列中接受系统治疗或生物治疗的银屑病患者的数据(英国皮肤科医师协会生物制剂和免疫调节剂登记处,BADBIR),通过绘制受试者工作特征曲线,确定基线疾病活动度改善90%(PASI 90)和75%(PASI 75)时的绝对PASI阈值。描述了PGA(清除、几乎清除、轻度、中度、中度 - 重度、重度)与PASI(范围0 - 72)之间的关系,并确定了反应的绝对定义和相对定义之间的一致性。采用相同方法基于PGA建立治疗反应和合格标准的定义。
有13422例患者的数据可用(58%为男性,91%为白种人,平均年龄44.9岁),包括超过23000个纵向PASI和PGA评分。在90%和88%的病例中,绝对PASI≤2分别与PASI 90一致,绝对PASI≤4分别与PASI 75一致。这些发现对于评估时间、基线疾病严重程度和治疗方式的亚组均具有稳健性。PASI和PGA高度相关(斯皮尔曼等级相关系数0.92)。对于PGA从清除到重度,PASI中位数分别从0(四分位间距0 - 0,范围0 - 23)增加到19(四分位间距15 - 25,范围0 - 64)。在90%的病例中,PGA清除/几乎清除与PASI≤2一致,在81%的病例中,PGA中度 - 重度/重度与英国国家卫生与临床优化研究所基于PASI的生物制剂合格标准一致。
绝对PASI≤2以及PGA清除/几乎清除代表了相关的疾病终点,可为银屑病的治疗达标管理策略提供依据。关于该主题已知的信息有哪些?银屑病中最常用的相对疾病活动度测量方法是银屑病面积和严重程度指数改善≥90%(PASI 90);然而,它有几个局限性,包括依赖基线严重程度评估。正如高血压和糖尿病等其他慢性病的治疗达标方法所表明的,在银屑病中定义绝对的目标疾病活动度终点有可能改善患者结局并降低成本。医生整体评估(PGA)是日常实践中常用的另一种银屑病严重程度测量方法;然而,其与PASI相关的效用尚未得到正式评估。本研究增加了什么内容?绝对PASI≤2与PASI 90反应相对应,是银屑病治疗达标方法的一个相关疾病终点。PASI和PGA之间存在高度相关性。PGA中度 - 重度/重度可作为基于PASI的生物制剂定义的替代合格标准,PGA清除/几乎清除是合适的替代绝对治疗终点。这项工作的临床意义是什么?绝对PASI≤2以及PGA清除/几乎清除代表了相关的疾病终点,可为银屑病的治疗达标管理策略提供依据。