Grande Roberta, Corsi Domenico, Mancini Raffaello, Gemma Donatello, Ciancola Fabrizio, Sperduti Isabella, Rossi Lorena, Fabbri Agnese, Diodoro Maria G, Ruggeri Enzo, Zampa Germano, Bianchetti Sara, Gamucci Teresa
Medical Oncology Unit-ASL Frosinone, Italy.
PLoS One. 2013 Dec 5;8(12):e80188. doi: 10.1371/journal.pone.0080188. eCollection 2013.
Adjuvant chemotherapy (AC) in Stage II Colon Cancer (CC) is still under debate. Choice should be based on patients and disease characteristics. According to guidelines AC should be considered in high-risk T3N0 patients. No data are available for better option in low-risk patients. The aim of the study is to retrospectively evaluate relapse-free survival (RFS) and disease-free survival (DFS) according to treatment received in T3N0 CC.
RFS and DFS are evaluated with Kaplan-Meier method. Multivariate Cox proportional hazard model was developed using stepwise regression, enter limit and remove limit were p = 0.10 and p = 0.15, respectively.
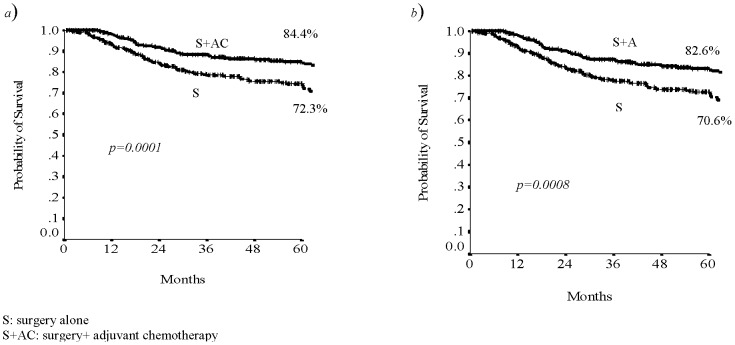
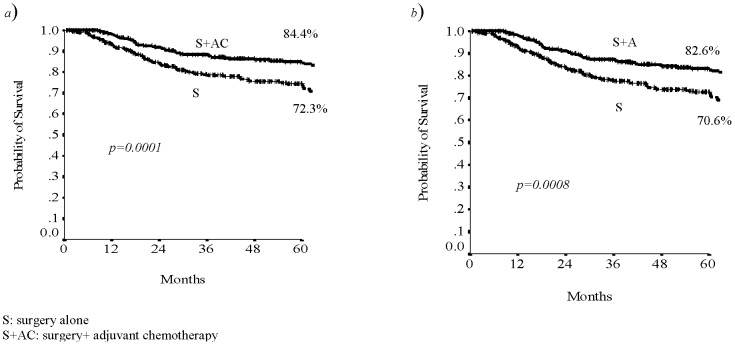
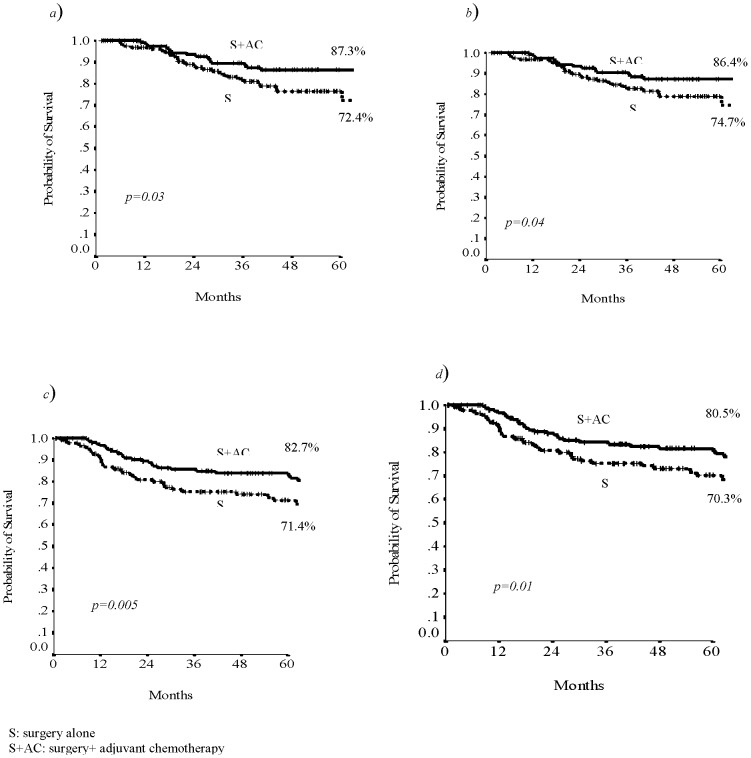
834 patients with T3N0 CC were recruited. Median age was 69 (29-93), M/F 463/371, 335 low-risk patients (40.2%), 387 high-risk (46.4%), 112 unknown (13.4%); 127 (15.2%) patients showed symptoms at diagnosis. Median sampled lymph nodes were 15 (1-76); 353 (42.3%) patients were treated with AC. Median follow up was 5 years (range 3-24). The 5-years RFS was 78.4% and the 5-years DFS was 76.7%. At multivariate analysis symptoms, lymph nodes, and adjuvant chemotherapy were prognostic factors for RFS. AC is prognostic factor for all endpoints. In low-risk group 5-years RFS was 87.3% in treated patients and 74.7% in non-treated patients (p 0.03); in high-risk group was respectively 82.7% and 71.4% (p 0.005).
Data confirmed the role of known prognostic factors and suggest the relevance of adjuvant chemotherapy also in low-risk stage II T3N0 CC patients. However, the highest risk in low-risk subgroup should be identified to be submitted to AC.
II期结肠癌(CC)的辅助化疗(AC)仍存在争议。治疗方案的选择应基于患者和疾病特征。根据指南,高危T3N0患者应考虑进行辅助化疗。目前尚无关于低危患者更佳治疗方案的数据。本研究的目的是根据T3N0期CC患者接受的治疗方法,回顾性评估无复发生存期(RFS)和无病生存期(DFS)。
采用Kaplan-Meier法评估RFS和DFS。使用逐步回归建立多变量Cox比例风险模型,纳入标准和剔除标准的p值分别为0.10和0.15。
共纳入834例T3N0期CC患者。中位年龄为69岁(29 - 93岁),男性463例,女性371例;335例低危患者(40.2%),387例高危患者(46.4%),112例情况不明患者(13.4%);127例(15.2%)患者在诊断时有症状。中位取样淋巴结数为15个(1 - 76个);353例(42.3%)患者接受了辅助化疗。中位随访时间为5年(范围3 - 24年)。5年RFS为78.4%,5年DFS为76.7%。多变量分析显示,症状、淋巴结和辅助化疗是RFS的预后因素。辅助化疗是所有终点的预后因素。在低危组中,接受治疗患者的5年RFS为87.3%,未接受治疗患者为74.7%(p = 0.03);在高危组中分别为82.7%和71.4%(p = 0.005)。
数据证实了已知预后因素的作用,并表明辅助化疗在低危II期T3N0 CC患者中也具有相关性。然而,应确定低危亚组中的最高风险患者,以便接受辅助化疗。