Department of Nephrology, Shuuwa General Hospital, 1200 Yaharashinden, Kasukabe, Saitama 344-0035, Japan.
BMC Nephrol. 2013 Dec 19;14:276. doi: 10.1186/1471-2369-14-276.
Hyponatremia is associated with increased mortality in chronic kidney disease with and without end-stage renal disease (ESRD). Increasing evidence suggests that hyponatremia is not only a marker of severe underlying disease, but also a direct contributor to mortality. However, specific pathogenesis or diseases contributing to mortality in the hyponatremic population are unknown. This study aimed to clarify the relationship between serum sodium level (sNa) and infection risk in ESRD patients.
This observational cohort study included 332 patients on maintenance hemodialysis in our dialysis unit in May 2009. The mean of 3 monthly measurements of glucose-corrected sNa before each dialysis session in May, June, and July 2009 was applied as baseline sNa. The primary endpoint was first infection-related hospitalization (IRH), and the secondary endpoint was death of any cause. Data were analyzed using Cox hazards modeling, adjusted for baseline demographics and characteristics, or laboratory data. Patients were followed until transfer, kidney transplantation, death, or study end on January 31, 2013.
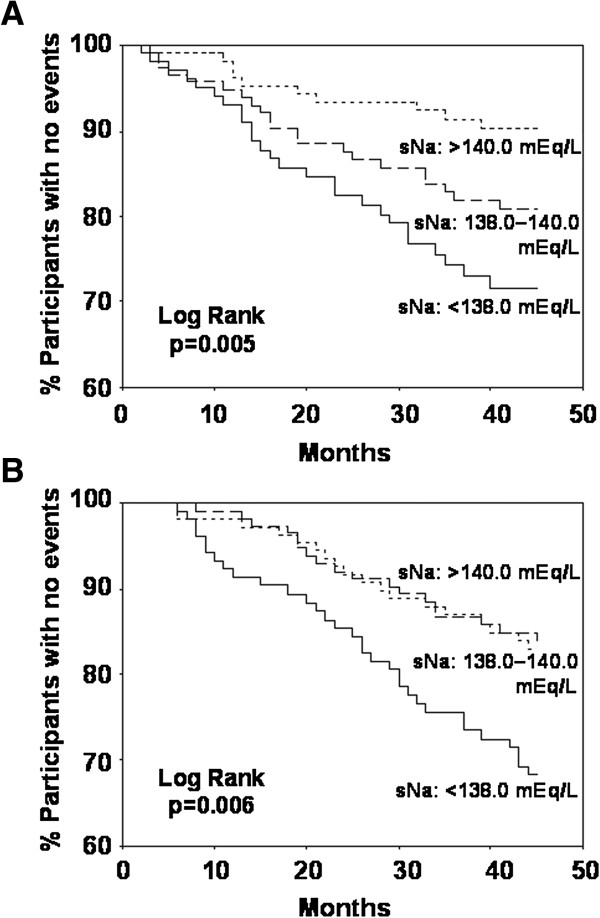
Mean sNa was 138.9 mEq/L (1st tertile: <138.0, n = 104; 2nd tertile: 138.0-140.0, n = 116; 3rd tertile: >140.0, n = 112). During 39.5 months' mean follow-up, 57 patients experienced IRH (56.4/1,000 patient-years overall; 89.7/1,000 in 1st tertile; 57.9/1,000 in 2nd tertile; 28.0/1,000 in 3rd tertile), and 68 patients died. The hazard ratio (HR) for IRH was higher for the 1st and 2nd tertiles than the 3rd tertile (unadjusted HR, 3.20; 95% confidence interval (CI), 1.54-6.64; p = 0.002; adjusted HR, 2.36; 95% CI, 1.10-5.04; p = 0.027; and unadjusted HR, 2.07; 95% CI, 0.98-4.40; p = 0.058; adjusted HR, 2.11; 95% CI, 0.99-4.51; p = 0.054 respectively). In a continuous model, higher sNa was associated with lower risk of IRH (adjusted HR, 0.90; 95% CI, 0.81-0.99; p = 0.040), and lower all-cause mortality (adjusted HR, 0.91; 95% CI, 0.83-1.00; p = 0.049).
Lower sNa is an independent predictor of higher risk for infection-related hospitalization in maintenance hemodialysis patients. Infectious disease may partially account for the increased mortality observed in the hyponatremic population with ESRD.
低钠血症与慢性肾脏病(CKD)合并或不合并终末期肾病(ESRD)患者的死亡率增加有关。越来越多的证据表明,低钠血症不仅是严重潜在疾病的标志物,也是导致死亡率增加的直接原因。然而,导致低钠血症人群死亡的具体发病机制或疾病尚不清楚。本研究旨在阐明 ESRD 患者血清钠水平(sNa)与感染风险之间的关系。
本观察性队列研究纳入了 2009 年 5 月在我院透析中心接受维持性血液透析的 332 例患者。将 2009 年 5 月、6 月和 7 月每次透析前 3 个月葡萄糖校正 sNa 的平均值作为基线 sNa。主要终点为首次感染相关住院(IRH),次要终点为任何原因导致的死亡。使用 Cox 风险模型分析数据,调整了基线人口统计学和特征或实验室数据。患者随访至 2013 年 1 月 31 日转移、肾移植、死亡或研究结束。
平均 sNa 为 138.9 mEq/L(1 分位数:<138.0,n=104;2 分位数:138.0-140.0,n=116;3 分位数:>140.0,n=112)。在 39.5 个月的平均随访期间,57 例患者发生 IRH(总体 1000 患者年发生率为 56.4/1000;1 分位数为 89.7/1000;2 分位数为 57.9/1000;3 分位数为 28.0/1000),68 例患者死亡。1 分位和 2 分位的 IRH 风险比(HR)高于 3 分位(未校正 HR,3.20;95%置信区间(CI),1.54-6.64;p=0.002;校正 HR,2.36;95%CI,1.10-5.04;p=0.027;未校正 HR,2.07;95%CI,0.98-4.40;p=0.058;校正 HR,2.11;95%CI,0.99-4.51;p=0.054)。在连续模型中,较高的 sNa 与较低的 IRH 风险相关(校正 HR,0.90;95%CI,0.81-0.99;p=0.040),较低的全因死亡率(校正 HR,0.91;95%CI,0.83-1.00;p=0.049)。
较低的 sNa 是维持性血液透析患者发生感染相关住院的独立预测因子。感染性疾病可能部分解释了 ESRD 合并低钠血症人群死亡率增加的原因。