*Tenon Hospital, Division of Infectious Diseases, Pierre and Marie Curie University, Paris, France; †Department of Epidemiology and ‡Division of Endocrinology and Metabolism, John Hopkins University, Baltimore, MD; §School of Medicine, Division of Infectious Diseases, University of Pittsburgh, Pittsburgh, PA; ‖L.A. Gay & Lesbian Center, Los Angeles, CA; and ¶Division of Infectious Diseases, Feinberg School of Medicine, Northwestern University, Chicago, IL.
J Acquir Immune Defic Syndr. 2014 Jan 1;65(1):57-64. doi: 10.1097/QAI.0b013e3182a99a0d.
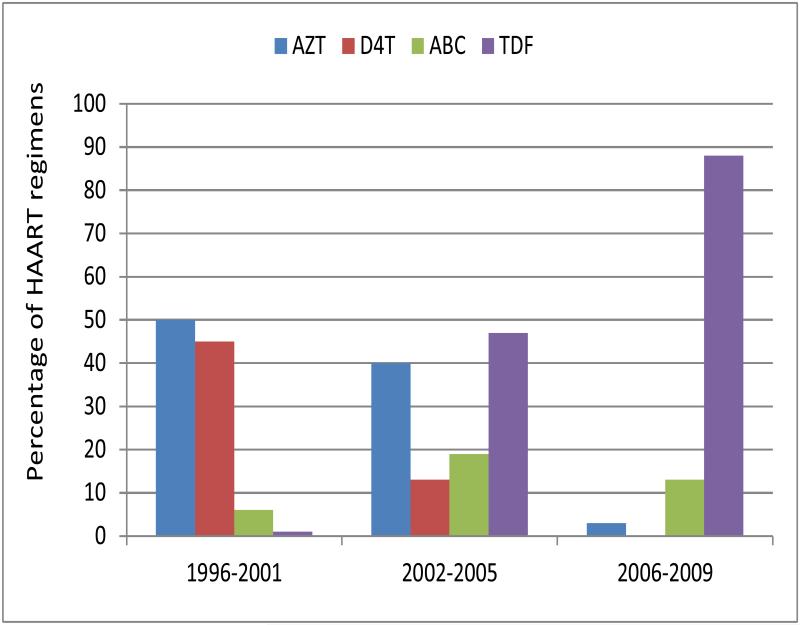
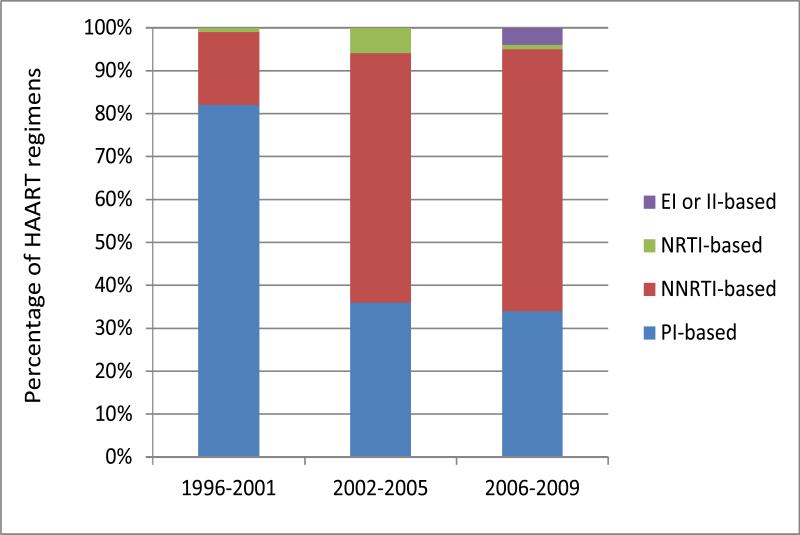
Antiretroviral therapy (ART) regimens changes occur frequently among HIV-infected persons. Duration and type of initial highly active antiretroviral therapy (HAART) and factors associated with regimen switching were evaluated in the Multicenter AIDS Cohort Study.
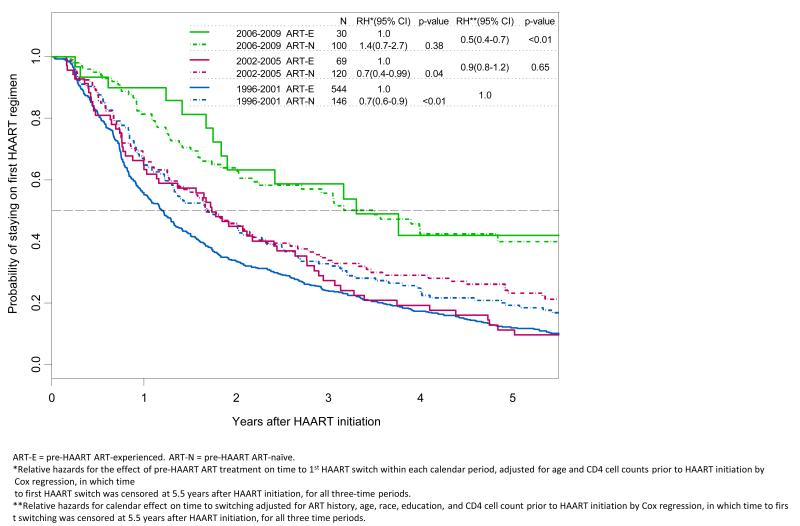
Participants were classified according to the calendar period of HAART initiation: T1 (1996-2001), T2 (2002-2005), and T3 (2006-2009). Kaplan-Meier curves depicted time from HAART initiation to first regimen changes within 5.5 years. Cox proportional hazards regression models were used to examine factors associated with time to switching.
Of 1009 participants, 796 changed regimen within 5.5 years after HAART initiation. The percentage of participants who switched declined from 85% during T1 to 49% in T3. The likelihood of switching in T3 decreased by 50% (P < 0.01) compared with T1 after adjustment for pre-HAART ART use, age, race, and CD4 count. Incomplete HIV suppression decreased over time (P < 0.01) but predicted switching across all time periods. Lower HAART adherence (≤95% of prescribed doses) was predictive of switching only in T1. In T2, central nervous system symptoms predicted switching [relative hazard (RH) = 1.7; P = 0.012]. Older age at HAART initiation was associated with increased switching in T1 (RH = 1.03 per year increase) and decreased switching in T2 (RH = 0.97 per year increase).
During the first 15 years of the HAART era, initial HAART regimen duration lengthened and regimen discontinuation rates diminished. Both HIV RNA nonsuppression and poor adherence predicted switching before 2001 while side effects that were possibly ART related were more prominent during T2.
在 HIV 感染者中,抗逆转录病毒疗法(ART)方案经常发生变化。本研究评估了多中心艾滋病队列研究中初始高效抗逆转录病毒治疗(HAART)的持续时间和类型以及与方案转换相关的因素。
根据 HAART 开始的日历时间将参与者分为 T1(1996-2001 年)、T2(2002-2005 年)和 T3(2006-2009 年)。Kaplan-Meier 曲线描绘了从 HAART 开始到 5.5 年内首次方案改变的时间。Cox 比例风险回归模型用于检查与时间相关的因素到切换。
在 1009 名参与者中,796 名在 HAART 开始后 5.5 年内改变了方案。参与者切换的百分比从 T1 期间的 85%下降到 T3 期间的 49%。在调整 HAART 治疗前、年龄、种族和 CD4 计数后,T3 时切换的可能性比 T1 降低了 50%(P < 0.01)。随着时间的推移,不完全 HIV 抑制减少(P < 0.01),但在所有时间段内都预测了切换。低 HAART 依从性(≤规定剂量的 95%)仅在 T1 时预测切换。在 T2 中,中枢神经系统症状预测切换[相对危险度(RH)= 1.7;P = 0.012]。HAART 开始时年龄较大与 T1 时的转换增加(RH = 每年增加 1.03)和 T2 时的转换减少(RH = 每年增加 0.97)相关。
在 HAART 时代的前 15 年,初始 HAART 方案的持续时间延长,方案中断率降低。在 2001 年之前,HIV RNA 非抑制和依从性差都预测了切换,而在 T2 期间,可能与 ART 相关的副作用更为突出。