Martinez-Vega Rosario, De La Mata Nicole L, Kumarasamy Nagalingeswaran, Ly Penh Sun, Van Nguyen Kinh, Merati Tuti P, Pham Thi Thanh, Lee Man Po, Choi Jun Yong, Ross Jeremy L, Ng Oon Tek
Department of Infectious Diseases, Institute of Infectious Diseases and Epidemiology, Tan Tock Seng Hospital, Singapore.
The Kirby Institute, UNSW Sydney, Sydney, NSW, Australia.
Antivir Ther. 2018;23(2):167-178. doi: 10.3851/IMP3194.
The durability of first-line regimen is important to achieve long-term treatment success for the management of HIV infection. Our analysis describes the duration of sequential ART regimens and identifies the determinants leading to treatment change in HIV-positive patients initiating in Asia.
All HIV-positive adult patients initiating first-line ART in 2003-2013, from eight clinical sites among seven countries in Asia. Patient follow-up was to May 2014. Kaplan-Meier curves were used to estimate the time to second-line ART and third-line ART regimen. Factors associated with treatment durability were assessed using Cox proportional hazards model.
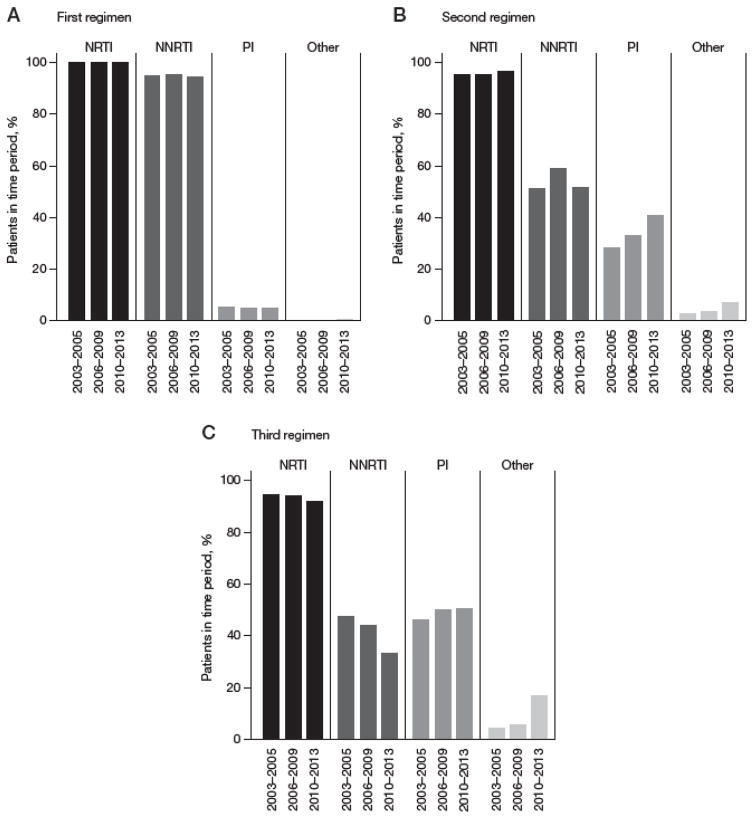
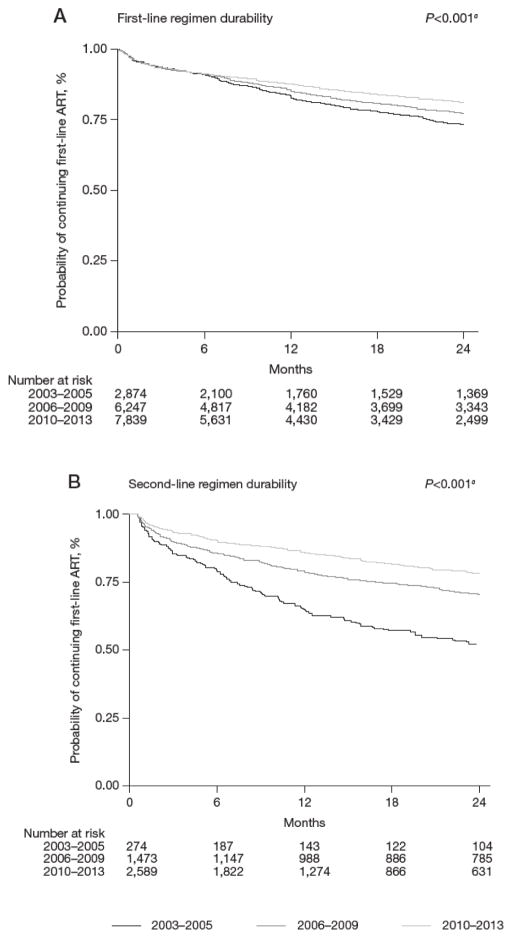
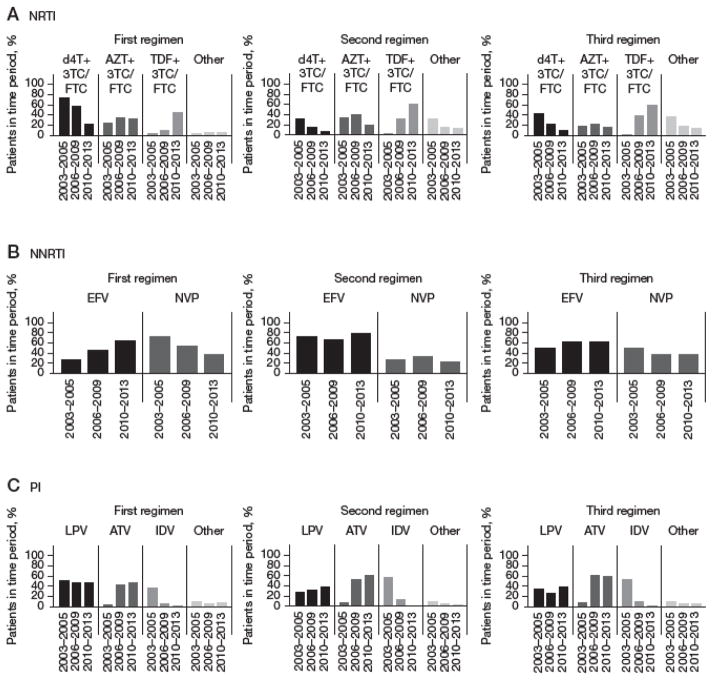
A total of 16,962 patients initiated first-line ART. Of these, 4,336 patients initiated second-line ART over 38,798 person-years (pys), a crude rate of 11.2 (95% CI 10.8, 11.5) per 100 pys. The probability of being on first-line ART increased from 83.7% (95% CI 82.1, 85.1%) in 2003-2005 to 87.9% (95% CI 87.1, 88.6%) in 2010-2013. Third-line ART was initiated by 1,135 patients over 8,078 pys, a crude rate of 14.0 (95% CI 13.3, 14.9) per 100 pys. The probability of continuing second-line ART significantly increased from 64.9% (95% CI 58.5, 70.6%) in 2003-2005 to 86.2% (95% CI 84.7, 87.6%) in 2010-2013.
Rates of discontinuation of first- and second-line regimens have decreased over the last decade in Asia. Subsequent regimens were of shorter duration compared to the first-line regimen initiated in the same year period. Lower CD4 T-cell count and the use of suboptimal regimens were important factors associated with higher risk of treatment switch.
一线治疗方案的持久性对于实现HIV感染管理的长期治疗成功至关重要。我们的分析描述了序贯抗逆转录病毒治疗方案的持续时间,并确定了导致亚洲开始治疗的HIV阳性患者治疗改变的决定因素。
2003年至2013年期间,来自亚洲七个国家的八个临床地点的所有开始一线抗逆转录病毒治疗的HIV阳性成年患者。患者随访至2014年5月。使用Kaplan-Meier曲线估计二线抗逆转录病毒治疗和三线抗逆转录病毒治疗方案的时间。使用Cox比例风险模型评估与治疗持久性相关的因素。
共有16962名患者开始一线抗逆转录病毒治疗。其中,4336名患者在38798人年(pys)内开始二线抗逆转录病毒治疗,粗发病率为每100 pys 11.2(95%CI 10.8,11.5)。接受一线抗逆转录病毒治疗的概率从2003-2005年的83.7%(95%CI 82.1,85.1%)增加到2010-2013年的87.9%(95%CI 87.1,88.6%)。1135名患者在8078 pys内开始三线抗逆转录病毒治疗,粗发病率为每100 pys 14.0(95%CI 13.3,14.9)。继续二线抗逆转录病毒治疗的概率从2003-2005年的64.9%(95%CI 58.5,70.6%)显著增加到2010-2013年的86.2%(95%CI 84.7,87.6%)。
在过去十年中,亚洲一线和二线治疗方案的停药率有所下降。与同年开始的一线治疗方案相比,后续治疗方案的持续时间较短。较低的CD4 T细胞计数和使用次优方案是与治疗转换风险较高相关的重要因素。