*Department of Thoracic Oncology, Lungen Clinic Großhansdorf, Großhansdorf, Germany; †Instituto de Biomedicina de Sevilla, University Hospital Virgen del Rocío, CSIC and Seville University, Seville, Spain; ‡San Camillo-Forlanini Hospital, Rome, Italy; §Le Mans Regional Hospital, Le Mans, France; ‖Jawaharlal Nehru Cancer Hospital and Research Center, Bhopal, India; ¶University Medical Center Hamburg-Eppendorf, Hamburg, Germany; #Eli Lilly and Company, Indianapolis, Indiana; **Eli Lilly and Company, Houten, The Netherlands; and ††Division of Medical Oncology, San Giuseppe Moscati Hospital, Avellino, Italy.
J Thorac Oncol. 2014 Feb;9(2):205-13. doi: 10.1097/JTO.0000000000000076.
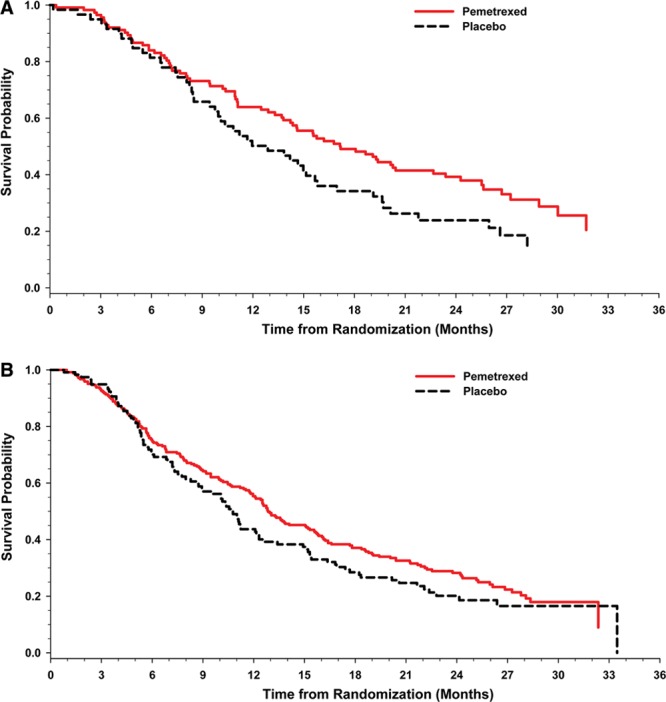
The PARAMOUNT phase III trial demonstrated that pemetrexed continuation maintenance significantly reduced the risk of disease progression (hazard ratio = 0.62) and death (hazard ratio = 0.78) versus placebo in patients with advanced nonsquamous non-small-cell lung cancer. To further understand the survival data, descriptive subgroup analyses were undertaken.
Nine hundred thirty-nine patients received induction therapy (four 21-day cycles pemetrexed 500 mg/m and cisplatin 75 mg/m), after which 539 nonprogressing patients with an Eastern Cooperative Oncology Group performance status (PS) of 0/1 were randomized (2:1) to maintenance pemetrexed (500 mg/m) cycles or placebo until disease progression.
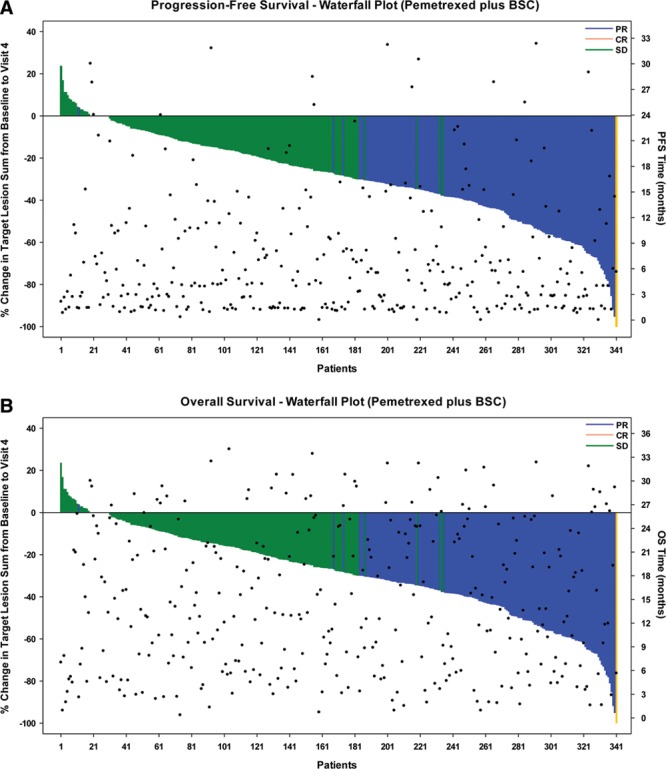
Baseline characteristics of patients surviving for longer periods were comparable to patients surviving shorter periods, suggesting overall survival (OS) benefit for all subgroups of patients on maintenance therapy. An examination of type and severity of induction adverse events also found no association with survival duration. Response to induction (tumor response versus stable disease) was not determinate of pemetrexed maintenance OS outcome as assessed by waterfall plot and scattergrams and by the distribution of patients among various OS intervals. The length of the interval before beginning maintenance therapy (<7 days versus ≥7/≤30 days) also did not impact the survival results. PS, a known prognostic factor, was the only baseline characteristic associated with improved OS; however, both PS 0 and PS 1 patients exhibited a survival benefit from pemetrexed maintenance.
In PARAMOUNT, the OS benefit was seen across all subgroups. Other than PS, no baseline or clinical parameter clearly identified a subgroup more likely to benefit. Maintenance treatment decisions should be made on an individual basis.
PARAMOUNT 三期试验表明,培美曲塞维持治疗可显著降低晚期非鳞状非小细胞肺癌患者疾病进展(风险比=0.62)和死亡(风险比=0.78)的风险,与安慰剂相比。为了进一步了解生存数据,进行了描述性亚组分析。
939 名患者接受了诱导治疗(培美曲塞 500mg/m 和顺铂 75mg/m,每 21 天 4 个周期),之后 539 名无进展的东部合作肿瘤学组(ECOG)表现状态(PS)为 0/1 的患者随机(2:1)接受培美曲塞(500mg/m)维持治疗或安慰剂,直至疾病进展。
存活时间较长的患者的基线特征与存活时间较短的患者相似,这表明维持治疗对所有亚组患者的总体生存(OS)都有获益。对诱导不良事件的类型和严重程度的检查也没有发现与生存时间有关。瀑布图和散点图评估以及根据患者在各种 OS 间隔的分布情况,对诱导反应(肿瘤反应与疾病稳定)与培美曲塞维持 OS 结果之间也没有关联。开始维持治疗前的间隔长度(<7 天与≥7/≤30 天)也没有影响生存结果。PS 是一个已知的预后因素,与 OS 改善有关;然而,PS 0 和 PS 1 患者均从培美曲塞维持治疗中获益。
在 PARAMOUNT 中,OS 获益见于所有亚组。除了 PS 之外,没有基线或临床参数能明确识别更有可能获益的亚组。维持治疗决策应根据个体情况做出。