Heigh Russell I, Yab Tracy C, Taylor William R, Hussain Fareeda T N, Smyrk Thomas C, Mahoney Douglas W, Domanico Michael J, Berger Barry M, Lidgard Graham P, Ahlquist David A
Division of Gastroenterology at Mayo Clinic, Scottsdale, Arizona, United States of America.
Division of Gastroenterology and Hepatology at Mayo Clinic, Rochester, Minnesota, United States of America.
PLoS One. 2014 Jan 20;9(1):e85659. doi: 10.1371/journal.pone.0085659. eCollection 2014.
Precursors to 1/3 of colorectal cancer (CRC), serrated polyps have been under-detected by screening due to their inconspicuous, non-hemorrhagic, and proximal nature. A new multi-target stool DNA test (multi-target sDNA) shows high sensitivity for both CRC and advanced adenomas. Screen detection of serrated polyps by this approach requires further validation. We sought to assess and compare noninvasive detection of sessile serrated polyps (SSP) ≥ 1 cm by sDNA and an occult blood fecal immunochemical test (FIT).
In a blinded prospective study, a single stool sample used for both tests was collected from 456 asymptomatic adults prior to screening or surveillance colonoscopy (criterion standard). All 29 patients with SSP ≥ 1 cm were included as cases and all 232 with no neoplastic findings as controls. Buffered stool samples were processed and frozen on receipt; Exact Sciences performed sDNA in batches using optimized analytical methods. The sDNA multi-marker panel targets methylated BMP3 (mBMP3) and NDRG4, mutant KRAS, β-actin, and hemoglobin. FIT (Polymedco OC-FIT Check) was performed in separate lab ≤ 2 days post defecation and evaluated at cutoffs of 50 (FIT-50) and 100 ng/ml (FIT-100).
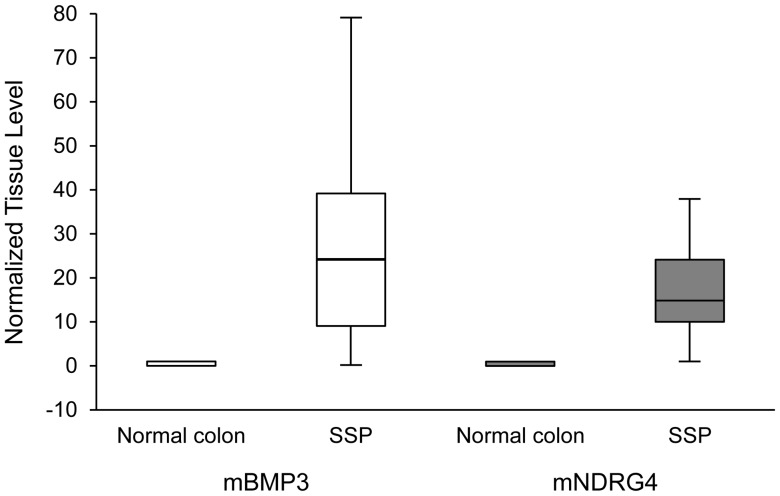
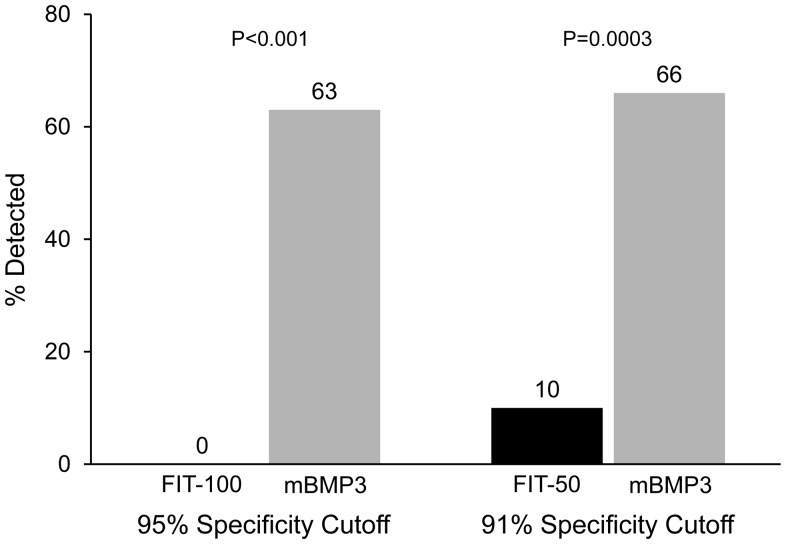
MEDIAN AGES: cases 61 (range 57-77), controls 62 (52-70), p = NS. Women comprised 59% and 51%, p = NS, respectively. SSP median size was 1.2 cm (1-3 cm), 93% were proximal, and 64% had synchronous diminutive polyps. Among multi-target sDNA markers, mBMP3 proved highly discriminant for detection of SSP ≥ 1 cm (AUC = 0.87, p<0.00001); other DNA markers provided no incremental sensitivity. Hemoglobin alone showed no discrimination (AUC = 0.50, p = NS). At matched specificities, detection of SSP ≥ 1 cm by stool mBMP3 was significantly greater than by FIT-50 (66% vs 10%, p = 0.0003) or FIT-100 (63% vs 0%, p<0.0001).
In a screening and surveillance setting, SSP ≥ 1 cm can be detected noninvasively by stool assay of exfoliated DNA markers, especially mBMP3. FIT appears to have no value in SSP detection.
锯齿状息肉是三分之一结直肠癌(CRC)的癌前病变,由于其不显眼、无出血且位置靠近近端,在筛查中未被充分检测到。一种新的多靶点粪便DNA检测(多靶点sDNA)对CRC和进展期腺瘤均显示出高灵敏度。通过这种方法对锯齿状息肉进行筛查检测需要进一步验证。我们试图评估和比较通过sDNA和粪便潜血免疫化学检测(FIT)对直径≥1 cm的无蒂锯齿状息肉(SSP)进行无创检测的效果。
在一项盲法前瞻性研究中,在进行筛查或监测结肠镜检查(标准参照)之前,从456名无症状成年人中采集用于两种检测的单一粪便样本。所有29例直径≥1 cm的SSP患者被纳入病例组,所有232例无肿瘤性病变的患者作为对照组。缓冲后的粪便样本在收到后进行处理并冷冻;Exact Sciences公司使用优化的分析方法分批进行sDNA检测。sDNA多标志物检测组合针对甲基化BMP3(mBMP3)、NDRG4、KRAS突变体、β-肌动蛋白和血红蛋白。FIT(Polymedco OC-FIT Check)在排便后≤2天在单独的实验室进行检测,并在50(FIT-50)和100 ng/ml(FIT-100)的临界值下进行评估。
中位年龄:病例组61岁(范围57 - 77岁),对照组62岁(52 - 70岁),p = 无显著差异。女性分别占59%和51%,p = 无显著差异。SSP的中位大小为1.2 cm(1 - 3 cm),93%位于近端,64%伴有同步微小息肉。在多靶点sDNA标志物中,mBMP3被证明对检测直径≥1 cm的SSP具有高度鉴别力(AUC = 0.87,p<0.00001);其他DNA标志物未提供额外的灵敏度。单独的血红蛋白无鉴别力(AUC = 0.50,p = 无显著差异)。在匹配的特异性下,粪便mBMP3检测直径≥1 cm的SSP的能力显著高于FIT-50(66%对10%,p = 0.0003)或FIT-100(63%对0%,p<0.0001)。
在筛查和监测环境中,通过对脱落DNA标志物进行粪便检测,尤其是mBMP3,可以无创检测直径≥1 cm的SSP。FIT在SSP检测中似乎没有价值。