Samuel Edward R, Beloki Lorea, Newton Katy, Mackinnon Stephen, Lowdell Mark W
Department of Haematology, University College London, Royal Free Campus, London, United Kingdom.
Oncohematology Research Group, Navarrabiomed-Miguel Servet Foundation, Pamplona, Spain.
PLoS One. 2014 Jan 17;9(1):e85911. doi: 10.1371/journal.pone.0085911. eCollection 2014.
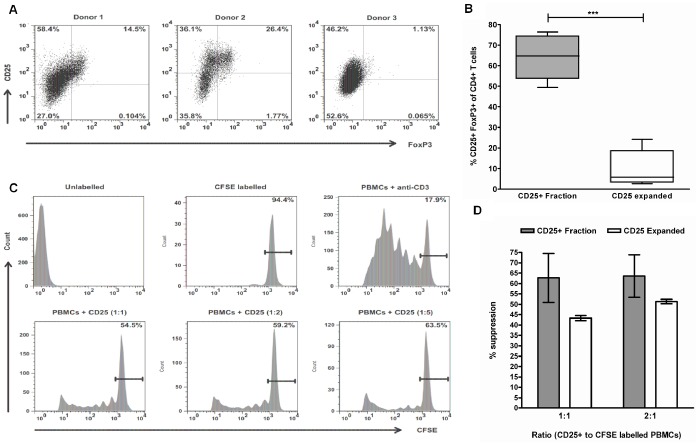
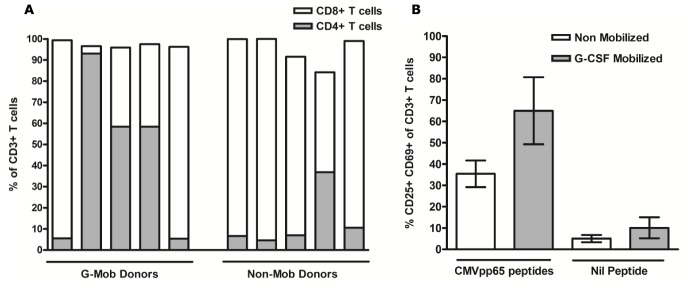
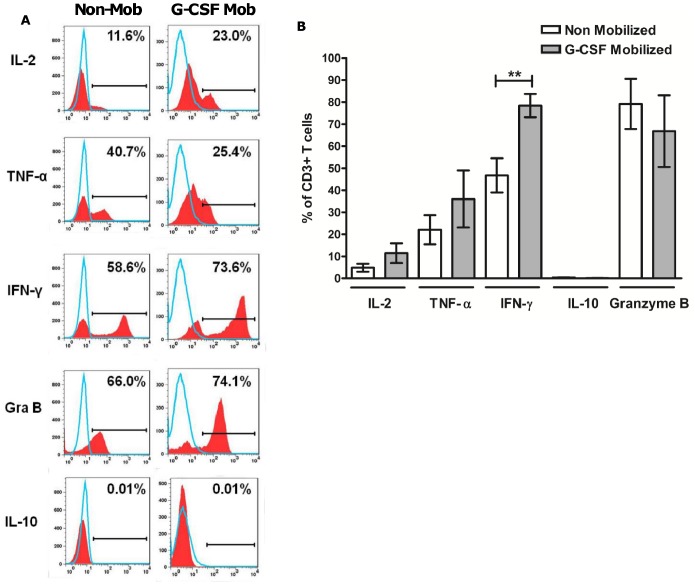
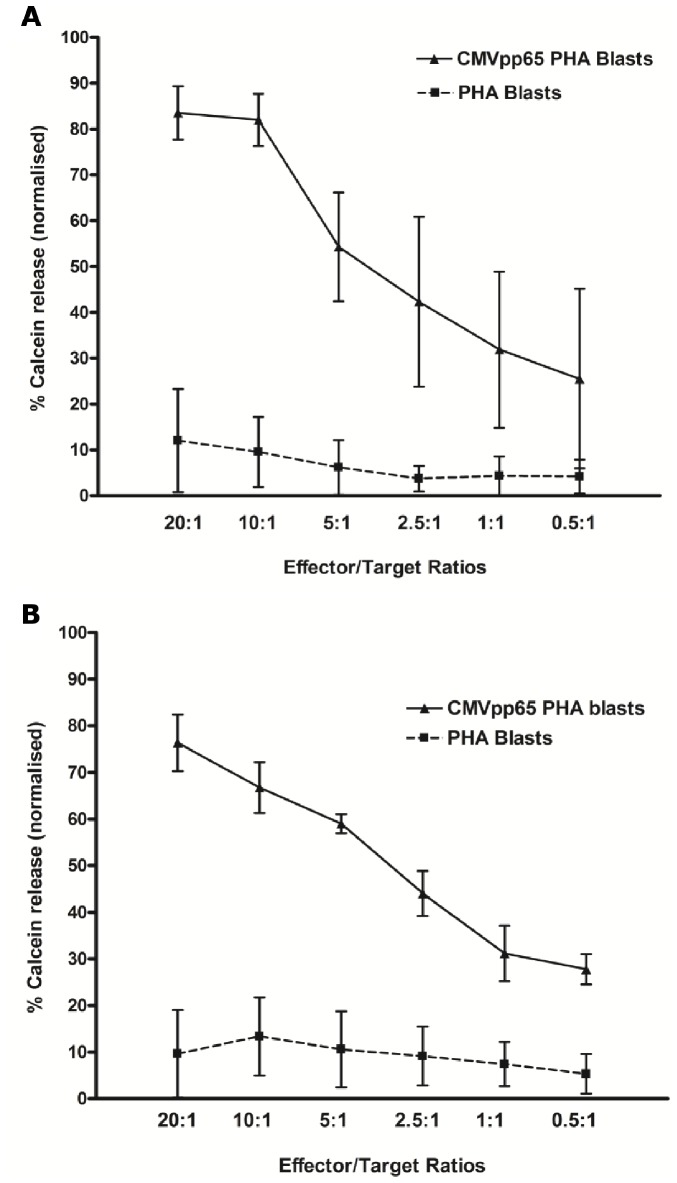
Previous studies have demonstrated the effective control of cytomegalovirus (CMV) infections post haematopoietic stem cell transplant through the adoptive transfer of donor derived CMV-specific T cells (CMV-T). Strategies for manufacturing CMV immunotherapies has involved a second leukapheresis or blood draw from the donor, which in the unrelated donor setting is not always possible. We have investigated the feasibility of using an aliquot of the original G-CSF-mobilized graft as a starting material for manufacture of CMV-T and examined the activation marker CD25 as a targeted approach for identification and isolation following CMVpp65 peptide stimulation. CD25+ cells isolated from G-CSF-mobilized apheresis revealed a significant increase in the proportion of FoxP3 expression when compared with conventional non-mobilized CD25+ cells and showed a superior suppressive capacity in a T cell proliferation assay, demonstrating the emergence of a population of Tregs not present in non-mobilized apheresis collections. The expansion of CD25+ CMV-T in short-term culture resulted in a mixed population of CD4+ and CD8+ T cells with CMV-specificity that secreted cytotoxic effector molecules and lysed CMVpp65 peptide-loaded phytohaemagglutinin-stimulated blasts. Furthermore CD25 expanded cells retained their suppressive capacity but did not maintain FoxP3 expression or secrete IL-10. In summary our data indicates that CD25 enrichment post CMV stimulation in G-CSF-mobilized PBMCs results in the simultaneous generation of both a functional population of anti-viral T cells and Tregs thus illustrating a potential single therapeutic strategy for the treatment of both GvHD and CMV reactivation following allogeneic haematopoietic stem cell transplantation. The use of G-CSF-mobilized cells as a starting material for cell therapy manufacture represents a feasible approach to alleviating the many problems incurred with successive donations and procurement of cells from unrelated donors. This approach may therefore simplify the clinical application of adoptive immunotherapy and broaden the approach for manufacturing multi-functional T cells.
先前的研究表明,通过过继转移供体来源的巨细胞病毒特异性T细胞(CMV-T),可有效控制造血干细胞移植后的巨细胞病毒(CMV)感染。制造CMV免疫疗法的策略涉及从供体进行第二次白细胞分离术或采血,而在无关供体的情况下,这并不总是可行的。我们研究了使用原始G-CSF动员的移植物的等分试样作为制造CMV-T的起始材料的可行性,并检查了活化标志物CD25,作为CMVpp65肽刺激后鉴定和分离的靶向方法。与传统的未动员的CD25 +细胞相比,从G-CSF动员的单采血液成分中分离出的CD25 +细胞显示FoxP3表达比例显著增加,并且在T细胞增殖试验中显示出更高的抑制能力,表明出现了未动员的单采血液成分中不存在的调节性T细胞群体。短期培养中CD25 + CMV-T的扩增产生了具有CMV特异性的CD4 +和CD8 + T细胞混合群体,这些细胞分泌细胞毒性效应分子并裂解负载CMVpp65肽的植物血凝素刺激的母细胞。此外,CD25扩增的细胞保留了其抑制能力,但未维持FoxP3表达或分泌IL-10。总之,我们的数据表明,G-CSF动员的外周血单个核细胞中CMV刺激后进行CD25富集可同时产生抗病毒T细胞和调节性T细胞的功能群体,从而说明了一种潜在的单一治疗策略,用于治疗异基因造血干细胞移植后的移植物抗宿主病(GvHD)和CMV再激活。使用G-CSF动员的细胞作为细胞治疗制造的起始材料是一种可行的方法,可缓解连续捐赠和从无关供体获取细胞所带来的许多问题。因此,这种方法可能会简化过继性免疫疗法的临床应用,并拓宽制造多功能T细胞的方法。