Department of Cardiothoracic Surgery and Anesthesiology, Karolinska University Hospital, Stockholm, Sweden ; Department of Molecular Medicine and Surgery, Karolinska Institutet, Stockholm, Sweden.
Department of Emergency Medicine, Karolinska University Hospital, Stockholm, Sweden ; Department of Internal Medicine, Karolinska Institutet, Stockholm, Sweden.
PLoS One. 2014 Jan 21;9(1):e86929. doi: 10.1371/journal.pone.0086929. eCollection 2014.
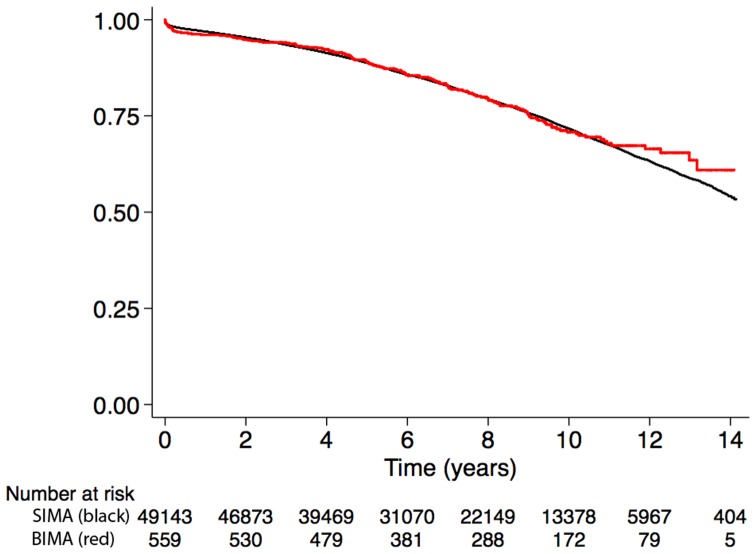
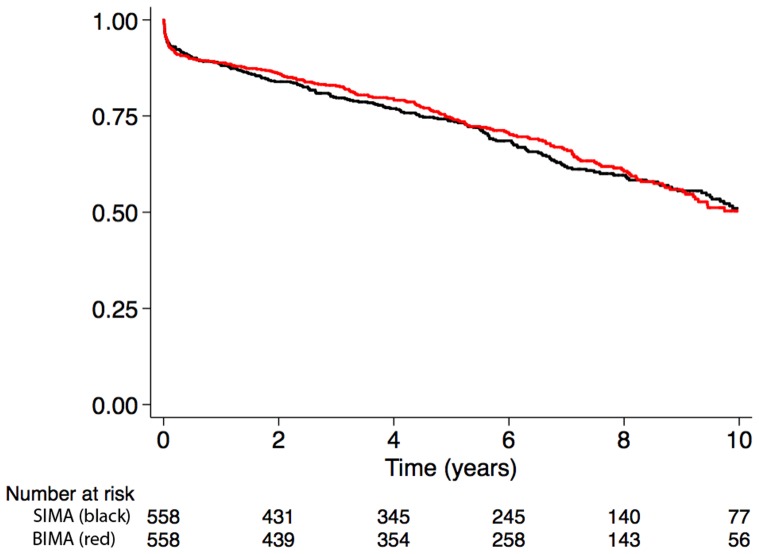
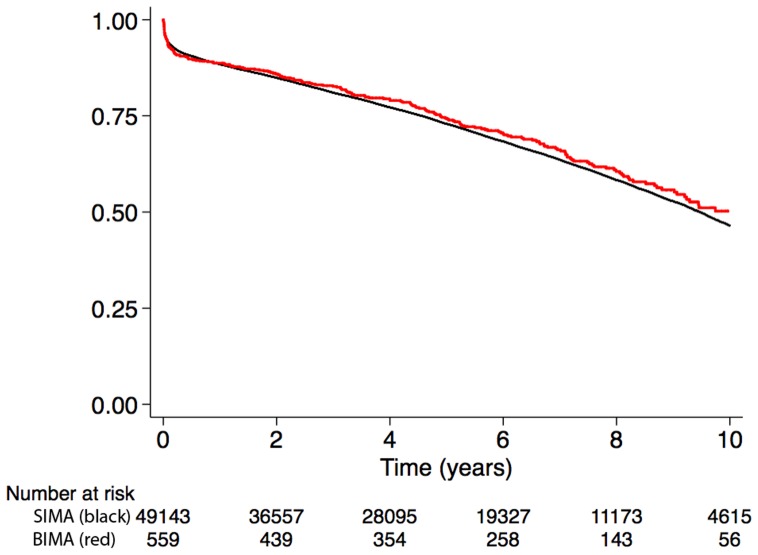
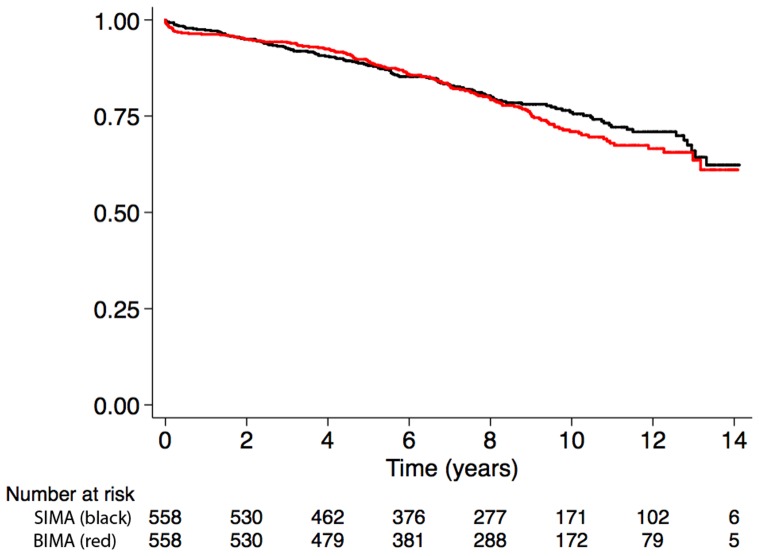
Prior observational studies have suggested better outcomes in patients who receive bilateral internal mammary arteries (BIMA) during coronary artery bypass grafting (CABG) compared with patients who receive a single internal mammary artery (SIMA). The aim of this study was to analyze the association between BIMA use and long-term survival in patients who underwent primary isolated CABG.
Patients who underwent primary isolated non-emergent CABG in Sweden between 1997 and 2008 were identified. The SWEDEHEART registry and other national Swedish registers were used to acquire information about patient characteristics and outcomes. Unadjusted and multivariable adjusted regression models were used to estimate the association between BIMA use and early mortality, long-term survival, and a composite of death from any cause or rehospitalization for myocardial infarction, heart failure, or stroke in the overall cohort and in a propensity score-matched cohort. The study population consisted of 49702 patients who underwent CABG with at least one internal mammary artery, and 559 (1%) of those had BIMA grafting. In the adjusted analyses, BIMA use was not associated with better survival compared with SIMA use in the overall cohort (hazard ratio (HR) for death: 1.16, 95% confidence interval (CI): 0.97 to 1.37) or in the matched cohort (HR: 1.04, 95% CI: 0.78 to 1.40). The results were similar for early mortality and the composite endpoint. Reoperation for sternal wound complications was more common among BIMA patients (odds ratio: 1.71, 95% CI: 1.01 to 2.88).
BIMA grafting was performed infrequently and was not associated with better outcomes compared with SIMA grafting in patients undergoing non-emergent primary isolated CABG in Sweden during 1997-2008.
先前的观察性研究表明,与接受单根内乳动脉(SIMA)的患者相比,在接受冠状动脉旁路移植术(CABG)时接受双侧内乳动脉(BIMA)的患者有更好的结局。本研究旨在分析 1997 年至 2008 年期间接受原发性非紧急 CABG 的患者中使用 BIMA 与长期生存之间的关联。
在瑞典,确定了 1997 年至 2008 年期间接受原发性非紧急 CABG 的患者。使用 SWEDEHEART 登记处和其他国家瑞典登记处获取有关患者特征和结局的信息。使用未调整和多变量调整回归模型来估计 BIMA 使用与早期死亡率、长期生存率以及全队列和倾向评分匹配队列中任何原因死亡或因心肌梗死、心力衰竭或中风再住院的复合终点之间的关联。研究人群包括 49702 例接受至少一根内乳动脉 CABG 的患者,其中 559 例(1%)接受了 BIMA 移植。在调整后的分析中,与 SIMA 相比,BIMA 使用与整体队列中的生存改善无关(死亡风险比:1.16,95%置信区间:0.97 至 1.37)或在匹配队列中(风险比:1.04,95%置信区间:0.78 至 1.40)。早期死亡率和复合终点的结果相似。BIMA 患者胸骨伤口并发症的再手术更为常见(比值比:1.71,95%置信区间:1.01 至 2.88)。
在 1997-2008 年期间,瑞典接受非紧急原发性孤立 CABG 的患者中,BIMA 移植的发生率较低,与 SIMA 移植相比,BIMA 移植并未带来更好的结局。