Department of Surgical Oncology, Netherlands Cancer Institute, Postbus 90203, 1006 BE, Amsterdam, The Netherlands.
Breast Cancer Res Treat. 2014 Feb;144(1):103-11. doi: 10.1007/s10549-013-2830-5. Epub 2014 Jan 28.
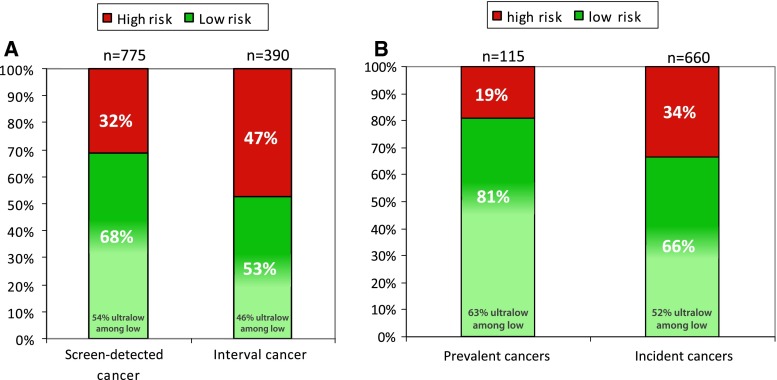
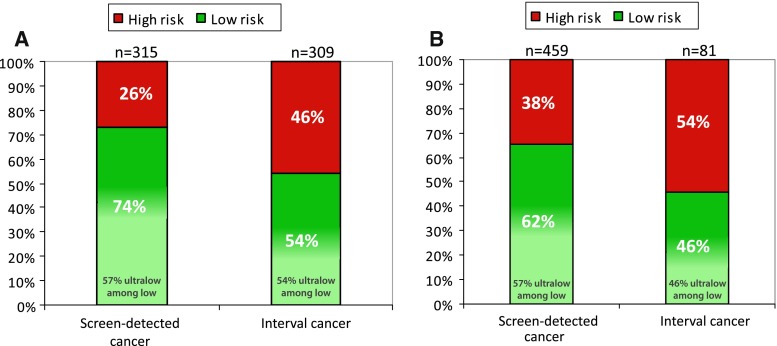
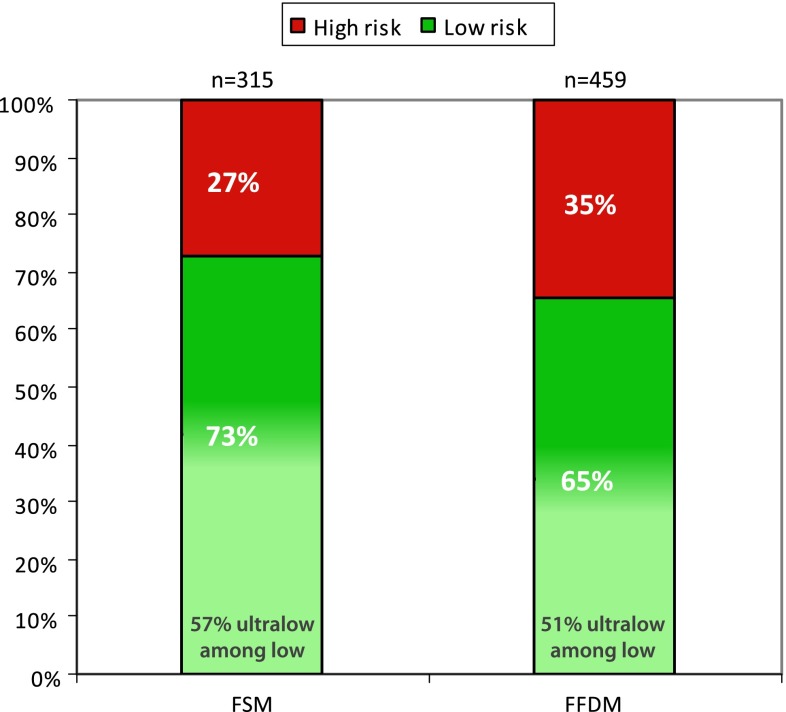
Overdiagnosis of breast cancer, i.e. the detection of slow-growing tumors that would never have caused symptoms or death, became more prevalent with the implementation of population-based screening. Only rough estimates have been made of the proportion of patients that are overdiagnosed and identification of those patients is difficult. Therefore, the aim of this study is to evaluate whether tumor biology can help identify patients with screen-detected tumors at such a low risk of recurrence that they are likely to be overdiagnosed. Furthermore, we wish to evaluate the impact of the transition from film-screen mammography (FSM) to the more sensitive full-field digital mammography (FFDM) on the biology of the tumors detected by each screening-modality. All Dutch breast cancer patients enrolled in the MINDACT trial (EORTC-10041) accrued 2007-2011, who participated in the national screening program (biennial screening ages 50-75) were included (n = 1,165). We calculated the proportions of high-, low- and among those the ultralow-risk tumors according to the 70-gene signature for patients with screen-detected (n = 775) and interval (n = 390) cancers for FSM and FFDM. Screen-detected cancers had significantly more often a low-risk tumor biology (68 %) of which 54 % even an ultralow-risk compared to interval cancers (53 % low-, of which 45 % ultralow-risk (p = 0.001) with an OR of 2.33 (p < 0.0001; 95 % CI 1.73-3.15). FFDM detected significantly more high-risk tumors (35 %) compared to FSM (27 %) (p = 0.011). Aside from favorable clinico-pathological factors, screen-detected cancers were also more likely to have a biologically low-risk or even ultralow-risk tumor. Especially for patients with screen-detected cancers the use of tools, such as the 70-gene signature, to differentiate breast cancers by risk of recurrence may minimize overtreatment. The recent transition in screening-modalities led to an increase in the detection of biologically high-risk cancers using FFDM.
乳腺癌的过度诊断,即检测到那些生长缓慢、永远不会引起症状或死亡的肿瘤,随着基于人群的筛查的实施变得更加普遍。只有对过度诊断患者的比例进行了粗略估计,而且很难识别这些患者。因此,本研究的目的是评估肿瘤生物学是否可以帮助识别那些由于复发风险极低而可能被过度诊断的筛查发现的肿瘤患者。此外,我们希望评估从胶片乳腺摄影(FSM)向更敏感的全数字化乳腺摄影(FFDM)的转变对每种筛查方式所检测到的肿瘤生物学的影响。所有于 2007-2011 年参加 MINDACT 试验(EORTC-10041)的荷兰乳腺癌患者,以及参加全国筛查计划(每两年筛查一次,年龄 50-75 岁)的患者都被纳入(n = 1,165)。我们根据 70 基因特征计算了 FSM 和 FFDM 中筛查发现(n = 775)和间隔期(n = 390)癌症患者中高危、低危和超低危肿瘤的比例。筛查发现的癌症中,低危肿瘤生物学比例显著更高(68%),其中 54%甚至是超低危(与间隔期癌症相比,53%为低危,其中 45%为超低危(p = 0.001),OR 为 2.33(p < 0.0001;95%CI 1.73-3.15)。FFDM 检测到的高危肿瘤比例明显高于 FSM(35%比 27%)(p = 0.011)。除了有利的临床病理因素外,筛查发现的癌症也更有可能具有生物学上的低危或超低危肿瘤。特别是对于筛查发现的癌症患者,使用 70 基因特征等工具根据复发风险来区分乳腺癌,可能会最大限度地减少过度治疗。最近筛查方式的转变导致使用 FFDM 检测到更多的生物学高危癌症。