Alistar Sabina S, Owens Douglas K, Brandeau Margaret L
Department of Management Science and Engineering, Stanford University, Stanford, California, United States of America.
Veterans Affairs Palo Healthcare System, Palo Alto, California, United States of America ; Center for Health Policy/Program on Clinical Outcomes Research, Stanford University, Stanford, California, United States of America.
PLoS One. 2014 Jan 28;9(1):e86584. doi: 10.1371/journal.pone.0086584. eCollection 2014.
Pre-exposure prophylaxis with oral antiretroviral treatment (oral PrEP) for HIV-uninfected injection drug users (IDUs) is potentially useful in controlling HIV epidemics with a significant injection drug use component. We estimated the effectiveness and cost effectiveness of strategies for using oral PrEP in various combinations with methadone maintenance treatment (MMT) and antiretroviral treatment (ART) in Ukraine, a representative case for mixed HIV epidemics.
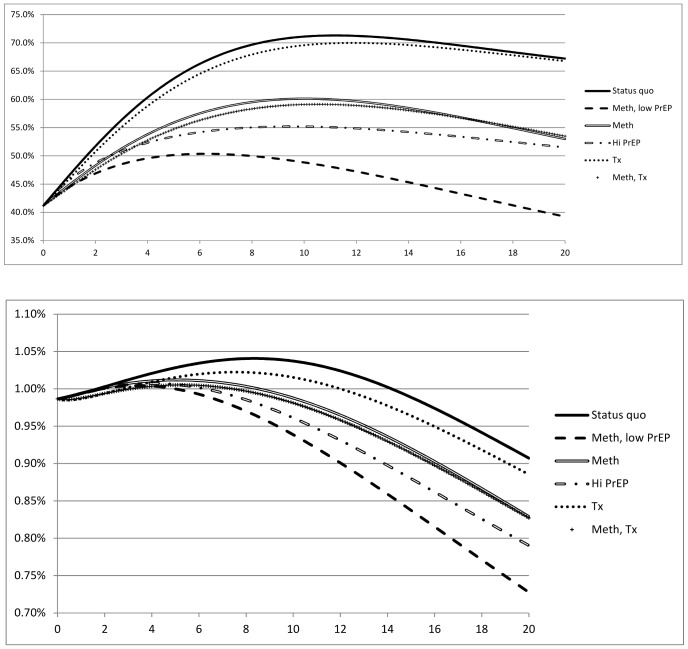
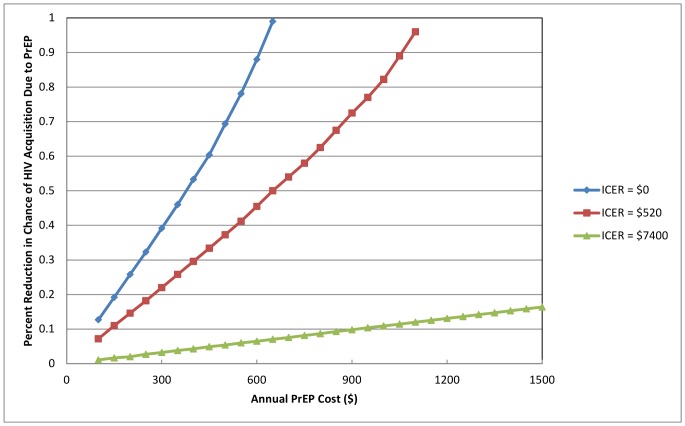
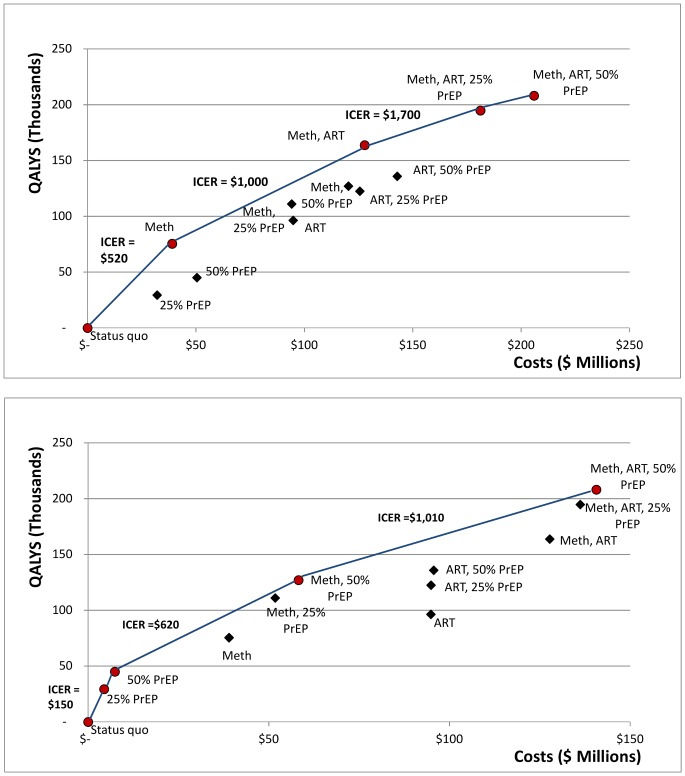
We developed a dynamic compartmental model of the HIV epidemic in a population of non-IDUs, IDUs who inject opiates, and IDUs in MMT, adding an oral PrEP program (tenofovir/emtricitabine, 49% susceptibility reduction) for uninfected IDUs. We analyzed intervention portfolios consisting of oral PrEP (25% or 50% of uninfected IDUs), MMT (25% of IDUs), and ART (80% of all eligible patients). We measured health care costs, quality-adjusted life years (QALYs), HIV prevalence, HIV infections averted, and incremental cost effectiveness. A combination of PrEP for 50% of IDUs and MMT lowered HIV prevalence the most in both IDUs and the general population. ART combined with MMT and PrEP (50% access) averted the most infections (14,267). For a PrEP cost of $950, the most cost-effective strategy was MMT, at $520/QALY gained versus no intervention. The next most cost-effective strategy consisted of MMT and ART, costing $1,000/QALY gained compared to MMT alone. Further adding PrEP (25% access) was also cost effective by World Health Organization standards, at $1,700/QALY gained. PrEP alone became as cost effective as MMT at a cost of $650, and cost saving at $370 or less.
Oral PrEP for IDUs can be part of an effective and cost-effective strategy to control HIV in regions where injection drug use is a significant driver of the epidemic. Where budgets are limited, focusing on MMT and ART access should be the priority, unless PrEP has low cost.
对于未感染艾滋病毒的注射吸毒者,采用口服抗逆转录病毒治疗进行暴露前预防(口服暴露前预防)可能有助于控制在注射吸毒占显著比例的艾滋病毒流行情况。我们估计了在乌克兰将口服暴露前预防与美沙酮维持治疗(MMT)和抗逆转录病毒治疗(ART)以各种组合方式使用的策略的有效性和成本效益,乌克兰是混合性艾滋病毒流行的一个典型案例。
我们建立了一个关于非注射吸毒者、注射阿片类药物的注射吸毒者以及接受美沙酮维持治疗的注射吸毒者人群中艾滋病毒流行情况的动态分区模型,并为未感染的注射吸毒者增加了一个口服暴露前预防项目(替诺福韦/恩曲他滨,易感性降低49%)。我们分析了由口服暴露前预防(25%或50%的未感染注射吸毒者)、美沙酮维持治疗(25%的注射吸毒者)和抗逆转录病毒治疗(80%的所有符合条件患者)组成的干预组合。我们衡量了医疗保健成本、质量调整生命年(QALYs)、艾滋病毒流行率、避免的艾滋病毒感染以及增量成本效益。50%的注射吸毒者接受暴露前预防与美沙酮维持治疗的组合在注射吸毒者和普通人群中降低艾滋病毒流行率的效果最为显著。抗逆转录病毒治疗与美沙酮维持治疗及暴露前预防(50%的覆盖率)相结合避免的感染最多(14267例)。对于暴露前预防成本为950美元的情况,最具成本效益的策略是美沙酮维持治疗,每获得一个质量调整生命年的成本为520美元,而不进行干预时则无此效益。次具成本效益的策略由美沙酮维持治疗和抗逆转录病毒治疗组成,与仅采用美沙酮维持治疗相比,每获得一个质量调整生命年的成本为1000美元。按照世界卫生组织的标准,进一步增加暴露前预防(25%的覆盖率)也是具有成本效益的,每获得一个质量调整生命年的成本为1700美元。当成本为650美元时,单独使用暴露前预防的成本效益与美沙酮维持治疗相当,成本低于或等于370美元时可节省成本。
在注射吸毒是疫情重要驱动因素的地区,为注射吸毒者提供口服暴露前预防可以成为控制艾滋病毒的有效且具有成本效益策略的一部分。在预算有限的情况下,除非暴露前预防成本较低,否则应优先关注美沙酮维持治疗和抗逆转录病毒治疗的可及性。