Department of Respiratory Medicine, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya 466-8550, Japan.
BMC Pulm Med. 2014 Feb 5;14:14. doi: 10.1186/1471-2466-14-14.
Recent studies suggest that coexistence of chronic obstructive pulmonary disease (COPD) might be independently related to a worse prognosis for lung cancer. However, because data on the substantial prevalence of COPD and its severity in Asian lung cancer patients remain limited, clinical impact of prevalence and severity of COPD among the population has not been fully evaluated. Furthermore, patients with COPD often have comorbidities. Thus, whether the decision-making process for therapeutic management of lung cancer patients might be independently affected by COPD remains elusive.
Clinical impact of prevalence and severity of COPD were evaluated in 270 Japanese patients with newly diagnosed lung cancer who were sequentially registered and underwent bronchoscopy from August 2010 to July 2012 at Nagoya University hospital. Furthermore, to explore whether or not the severity of airflow obstruction might affect the decision to propose thoracic surgery with curative intent, we evaluated data from patients with lung cancer at stage 1A to 3A who underwent spirometry and bronchoscopy.
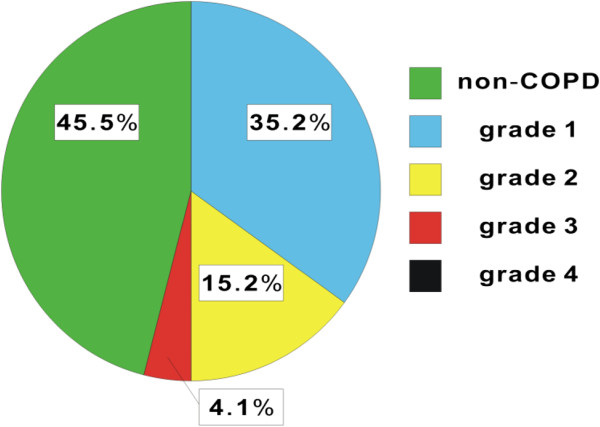
The prevalence rate of COPD was 54.4% among Japanese patients with lung cancer who underwent bronchoscopy. The incidence of Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades 1 and 2 was significantly higher than that of GOLD grade 3. Although COPD-related comorbidities were not independent factors for proposing thoracic surgery, the number of thoracic surgeries performed was significantly less in the COPD group than the non-COPD group. Multivariate analysis showed that more severe airway obstruction, advanced clinical staging, and higher age, were independent factors associated with the decision on thoracic surgery.
We demonstrated a high prevalence of COPD among Japanese lung cancer patients. Based on the knowledge that severity of COPD is one of the most important factors in the therapeutic decision, comprehensive assessment of COPD at bronchoscopy might allow us to implement the optimum management for lung cancer patients.
最近的研究表明,慢性阻塞性肺疾病(COPD)的共存可能与肺癌的预后较差独立相关。然而,由于亚洲肺癌患者中 COPD 的患病率和严重程度的数据仍然有限,因此 COPD 的患病率和严重程度对人群的临床影响尚未得到充分评估。此外,COPD 患者常有合并症。因此,COPD 是否会独立影响肺癌患者的治疗管理决策过程仍不清楚。
对 270 例在名古屋大学医院接受支气管镜检查的新诊断肺癌日本患者的 COPD 患病率和严重程度的临床影响进行了评估。此外,为了探讨气流阻塞的严重程度是否会影响提出有治愈意图的胸外科手术的决策,我们评估了在接受支气管镜检查的 1A 期至 3A 期肺癌患者中的数据。
接受支气管镜检查的日本肺癌患者中 COPD 的患病率为 54.4%。全球慢性阻塞性肺疾病倡议(GOLD)1 级和 2 级的发生率明显高于 GOLD 3 级。尽管 COPD 相关合并症不是提出胸外科手术的独立因素,但 COPD 组的胸外科手术数量明显少于非 COPD 组。多变量分析显示,气道阻塞更严重、临床分期更晚以及年龄更大是与胸外科手术决策相关的独立因素。
我们表明日本肺癌患者中 COPD 的患病率很高。基于 COPD 严重程度是治疗决策中最重要因素之一的知识,在支气管镜检查时对 COPD 进行全面评估可能使我们能够为肺癌患者实施最佳管理。