Mogensen Trine H, Bernth-Jensen Jens Magnus, Petersen Charlotte C, Petersen Mikkel S, Nyvold Charlotte, Gadegaard Karsten H, Hokland Marianne, Hokland Peter, Larsen Carsten S
Department of Infectious Diseases, Aarhus University Hospital, Skejby Brendstrupgaardsvej, DK-8200, Aarhus N, Denmark.
BMC Hematol. 2013 Apr 11;13(1):4. doi: 10.1186/2052-1839-13-4.
Hypogammaglobulinemia may be part of several different immunological or malignant conditions, and its origin is not always obvious. Furthermore, although autoimmune cytopenias are known to be associated with common variable immunodeficiency (CVID) and even may precede signs of immunodeficiency, this is not always recognized. Despite novel insight into the molecular immunology of common variable immunodeficiency, several areas of uncertainty remain. In addition, the full spectrum of immunological effects of the B cell depleting anti-CD20 antibody Rituximab has not been fully explored. To our knowledge this is the first report of development of CVID in a patient with normal immunoglobulin prior to Rituximab treatment.
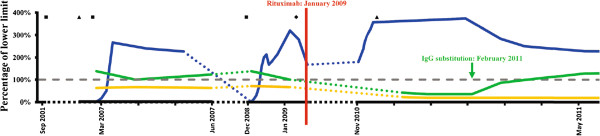
Here we describe the highly unusual clinical presentation of a 34-year old Caucasian male with treatment refractory immune thrombocytopenic purpura and persistent lymphadenopathy, who was splenectomized and received multiple courses of high-dose corticosteroid before treatment with Rituximab resulted in a sustained response. However, in the setting of severe pneumococcal meningitis, hypogammaglobulinemia was diagnosed. An extensive immunological investigation was performed in order to characterize his immune status, and to distinguish between a primary immunodeficiency and a side effect of Rituximab treatment. We provide an extensive presentation and discussion of the literature on the basic immunology of CVID, the mechanism of action of Rituximab, and the immunopathogenesis of hypogammaglobulinemia observed in this patient.
We suggest that CVID should be ruled out in any patient with immune cytopenias in order to avoid diagnostic delay. Likewise, we stress the importance of monitoring immunoglobulin levels before, during, and after Rituximab therapy to identify patients with hypogammaglobulinemia to ensure initiation of immunoglobulin replacement therapy in order to avoid life-threatening invasive bacterial infections. Recent reports indicate that Rituximab is not contra-indicated for the treatment of CVID-associated thrombocytopenia, however concomitant immunoglobulin substitution therapy is of fundamental importance to minimize the risk of infections. Therefore, lessons can be learned from this case report by clinicians caring for patients with immunodeficiencies, haematological diseases or other autoimmune disorders, particularly, when Rituximab treatment may be considered.
低丙种球蛋白血症可能是几种不同免疫或恶性疾病的一部分,其起源并不总是显而易见。此外,虽然自身免疫性血细胞减少症已知与常见可变免疫缺陷(CVID)相关,甚至可能先于免疫缺陷症状出现,但这并不总是被认识到。尽管对常见可变免疫缺陷的分子免疫学有了新的认识,但仍存在一些不确定的领域。此外,B细胞耗竭性抗CD20抗体利妥昔单抗的全部免疫效应尚未得到充分探索。据我们所知,这是第一例在利妥昔单抗治疗前免疫球蛋白正常的患者发生CVID的报告。
在此,我们描述了一名34岁白种男性的高度不寻常的临床表现,该患者患有治疗难治性免疫性血小板减少性紫癜和持续性淋巴结病,在接受利妥昔单抗治疗获得持续缓解之前,他接受了脾切除术并接受了多个疗程的高剂量皮质类固醇治疗。然而,在严重肺炎球菌脑膜炎的情况下,诊断出低丙种球蛋白血症。进行了广泛的免疫学调查,以表征他的免疫状态,并区分原发性免疫缺陷和利妥昔单抗治疗的副作用。我们对关于CVID的基础免疫学、利妥昔单抗的作用机制以及在该患者中观察到的低丙种球蛋白血症的免疫发病机制的文献进行了广泛的介绍和讨论。
我们建议,对于任何患有免疫性血细胞减少症的患者,都应排除CVID,以避免诊断延误。同样,我们强调在利妥昔单抗治疗前、治疗期间和治疗后监测免疫球蛋白水平的重要性,以识别低丙种球蛋白血症患者,确保开始免疫球蛋白替代治疗,以避免危及生命的侵袭性细菌感染。最近的报告表明,利妥昔单抗并非治疗CVID相关血小板减少症的禁忌药物,然而,同时进行免疫球蛋白替代治疗对于将感染风险降至最低至关重要。因此,照顾免疫缺陷、血液系统疾病或其他自身免疫性疾病患者的临床医生可以从本病例报告中吸取经验教训,特别是在考虑使用利妥昔单抗治疗时。