Gupta Ravindra K, Marks Michael, Edwards Simon G, Smith Katie, Fletcher Katie, Lee Siow-Ming, Ramsay Alan, Copas Andrew J, Miller Robert F
Division of Infection and Immunity, University College London, London, United Kingdom ; University College London Hospitals' NHS Foundation Trust, London, United Kingdom.
University College London Hospitals' NHS Foundation Trust, London, United Kingdom ; Clinical Research Department, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom.
PLoS One. 2014 Feb 4;9(2):e87442. doi: 10.1371/journal.pone.0087442. eCollection 2014.
The incidence of Hodgkin lymphoma (HL) among HIV-infected individuals remains unchanged since the introduction of combination antiretroviral therapy (cART). Recent epidemiological data suggest that CD4 count decline over a year is associated with subsequent diagnosis of HL. In an era of economic austerity monitoring the efficacy of cART by CD4 counts may no longer be required where CD4 count>350 cells/µl and viral load is suppressed (<50 copies/ml).
We sought to establish among our HIV outpatient cohort whether a CD4 count decline prior to diagnosis of HL, whether any decline was greater than in patients without the diagnosis, and also whether other clinical or biochemical indices were reliably associated with the diagnosis.
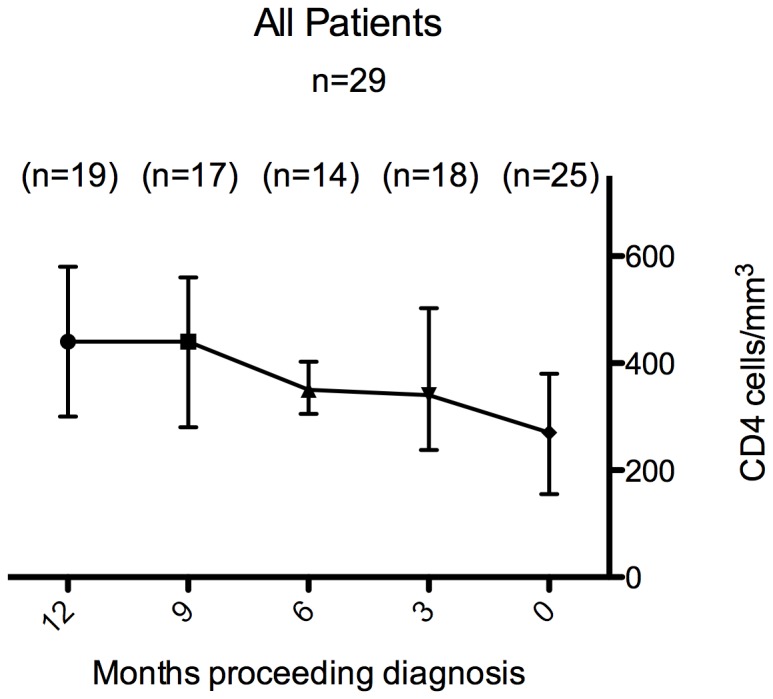
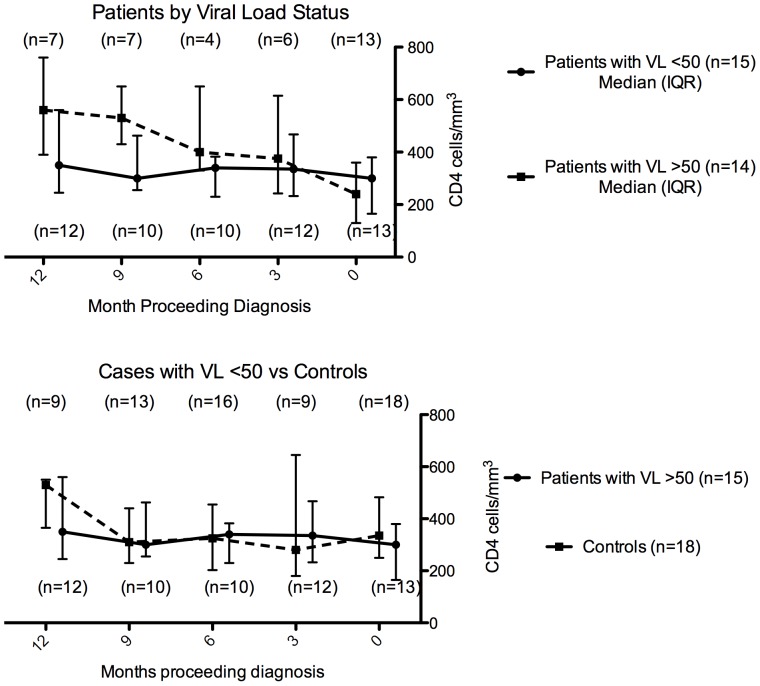
Twenty-nine patients with a diagnosis of HL were identified. Among 15 individuals on cART with viral load <50 copies/ml the change in CD4 over 12 months preceding diagnosis of HL was -82 cells/µl (95% CI -163 to -3; p = 0.04). Among 18 matched controls the mean change was +5 cells/µl, 95% CI -70 to 80, p = 0.89). The decline in CD4 over the previous 6-12 months was somewhat greater in cases than controls (mean difference in change -55 cells/µl, 95% CI -151 to 39; p = 0.25). In 26 (90%) patients B symptoms had been present for a median of three months (range one-12) before diagnosis of HL.
The CD4 count decline in the 12 months prior to diagnosis of Hodgkin lymphoma among HIV-infected individuals with VL<50 copies/ml on cART was not significantly different from that seen in other fully virologically suppressed individuals in receipt of cART and who did not develop HL. All those who developed HL had B symptoms and/or new palpable lymphadenopathy, suggesting that CD4 count monitoring if performed less frequently, or not at all, among those virologically suppressed individuals with CD4 counts >350 may not have delayed diagnosis.
自联合抗逆转录病毒疗法(cART)引入以来,HIV感染者中霍奇金淋巴瘤(HL)的发病率保持不变。近期的流行病学数据表明,一年内CD4细胞计数下降与随后HL的诊断相关。在经济紧缩的时代,当CD4细胞计数>350个/微升且病毒载量得到抑制(<50拷贝/毫升)时,通过CD4细胞计数监测cART疗效可能不再必要。
我们试图在HIV门诊队列中确定HL诊断前CD4细胞计数是否下降,下降幅度是否大于未诊断患者,以及其他临床或生化指标是否与该诊断可靠相关。
确定了29例HL诊断患者。在15例接受cART且病毒载量<50拷贝/毫升的患者中,HL诊断前12个月CD4细胞计数变化为-82个/微升(95%置信区间-163至-3;p = 0.04)。在18例匹配对照中,平均变化为+5个/微升,95%置信区间-70至80,p = 0.89)。病例组前6至12个月CD4细胞计数下降幅度略大于对照组(变化平均差异-55个/微升,95%置信区间-151至39;p = 0.25)。26例(90%)患者在HL诊断前B症状出现的中位时间为3个月(范围1至12个月)。
在接受cART且病毒载量<50拷贝/毫升的HIV感染者中,HL诊断前12个月的CD4细胞计数下降与接受cART且病毒学完全抑制但未发生HL的其他个体相比无显著差异。所有发生HL的患者均有B症状和/或新出现的可触及淋巴结肿大,这表明在病毒学抑制且CD4细胞计数>350的个体中,若减少CD4细胞计数监测频率或根本不进行监测,可能不会延迟诊断。