Harvard Medical School, Boston, MASection of General Internal Medicine, VA Boston Healthcare System, Boston, MADivision of General Internal Medicine and Primary Care, Brigham and Women's Hospital, Boston, MA.
Harvard Medical School, Boston, MADepartment of Population Medicine, Harvard Pilgrim Health Care Institute, Boston, MADivision of Endocrinology, Department of Medicine, Université de Sherbrooke, Sherbrooke, Quebec, Canada.
Diabetes. 2014 Jun;63(6):2172-82. doi: 10.2337/db13-1663. Epub 2014 Feb 11.
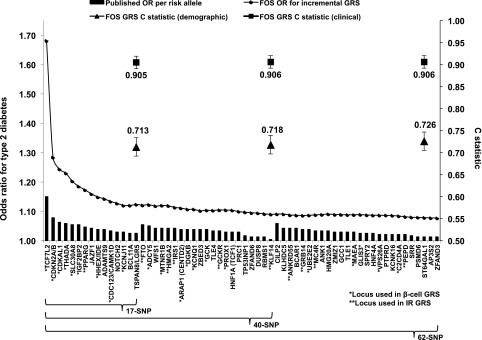
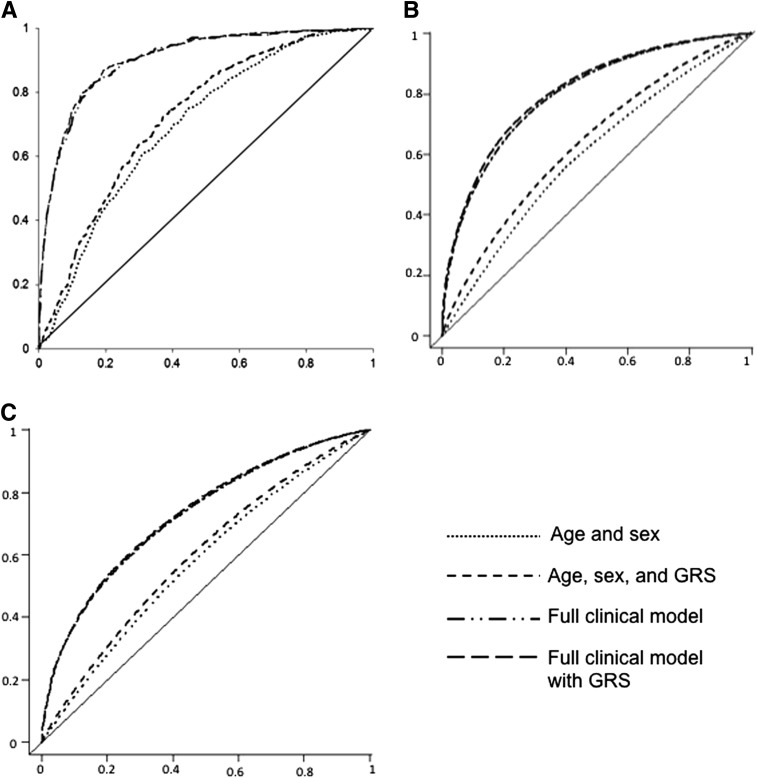
Genome-wide association studies (GWAS) may have reached their limit of detecting common type 2 diabetes (T2D)-associated genetic variation. We evaluated the performance of current polygenic T2D prediction. Using data from the Framingham Offspring (FOS) and the Coronary Artery Risk Development in Young Adults (CARDIA) studies, we tested three hypotheses: 1) a 62-locus genotype risk score (GRSt) improves T2D prediction compared with previous less inclusive GRSt; 2) separate GRS for β-cell (GRSβ) and insulin resistance (GRSIR) independently predict T2D; and 3) the relationships between T2D and GRSt, GRSβ, or GRSIR do not differ between blacks and whites. Among 1,650 young white adults in CARDIA, 820 young black adults in CARDIA, and 3,471 white middle-aged adults in FOS, cumulative T2D incidence was 5.9%, 14.4%, and 12.9%, respectively, over 25 years. The 62-locus GRSt was significantly associated with incident T2D in all three groups. In FOS but not CARDIA, the 62-locus GRSt improved the model C statistic (0.698 and 0.726 for models without and with GRSt, respectively; P < 0.001) but did not materially improve risk reclassification in either study. Results were similar among blacks compared with whites. The GRSβ but not GRSIR predicted incident T2D among FOS and CARDIA whites. At the end of the era of common variant discovery for T2D, polygenic scores can predict T2D in whites and blacks but do not outperform clinical models. Further optimization of polygenic prediction may require novel analytic methods, including less common as well as functional variants.
全基因组关联研究(GWAS)可能已经达到了检测常见 2 型糖尿病(T2D)相关遗传变异的极限。我们评估了当前多基因 T2D 预测的性能。使用 Framingham 后代(FOS)和冠状动脉风险发展在年轻人(CARDIA)研究的数据,我们测试了三个假设:1)62 个基因座基因型风险评分(GRSt)比以前的包容性较小的 GRSt 提高了 T2D 预测;2)单独的β细胞(GRSβ)和胰岛素抵抗(GRSIR)的 GRS 独立预测 T2D;3)T2D 与 GRSt、GRSβ 或 GRSIR 之间的关系在黑人和白人之间没有差异。在 CARDIA 的 1650 名年轻白人成年人、CARDIA 的 820 名年轻黑人成年人和 FOS 的 3471 名白人中年成年人中,累积 T2D 发病率分别为 5.9%、14.4%和 12.9%,随访时间为 25 年。在所有三组人群中,62 个基因座 GRSt 与 T2D 发病显著相关。在 FOS 中,但不是在 CARDIA 中,62 个基因座 GRSt 提高了模型 C 统计量(无和有 GRSt 的模型分别为 0.698 和 0.726;P<0.001),但在这两项研究中都没有显著改善风险再分类。黑人中的结果与白人相似。在 FOS 和 CARDIA 的白人中,GRSβ 而不是 GRSIR 预测了 T2D 的发病。在 T2D 常见变异发现的时代末期,多基因评分可以预测白人和黑人的 T2D,但不能优于临床模型。多基因预测的进一步优化可能需要新的分析方法,包括不常见的和功能变异。