School of Medicine, The University of Queensland, Australia.
Department of Dermatology, Division of General Dermatology, Medical University of Vienna, Austria.
Dermatol Pract Concept. 2014 Jan 31;4(1):59-66. doi: 10.5826/dpc.0401a09. eCollection 2014 Jan.
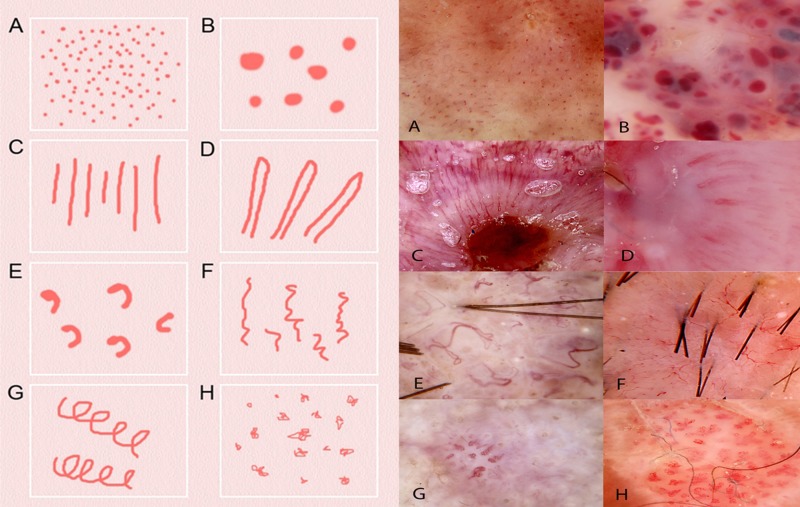
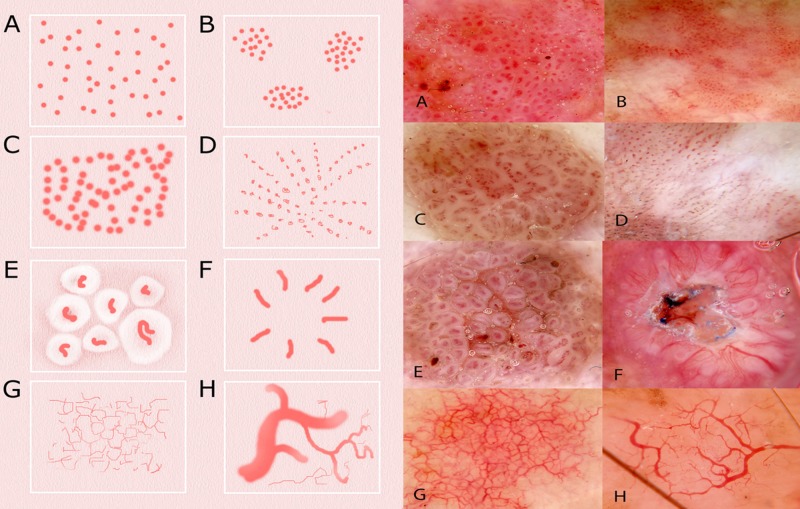
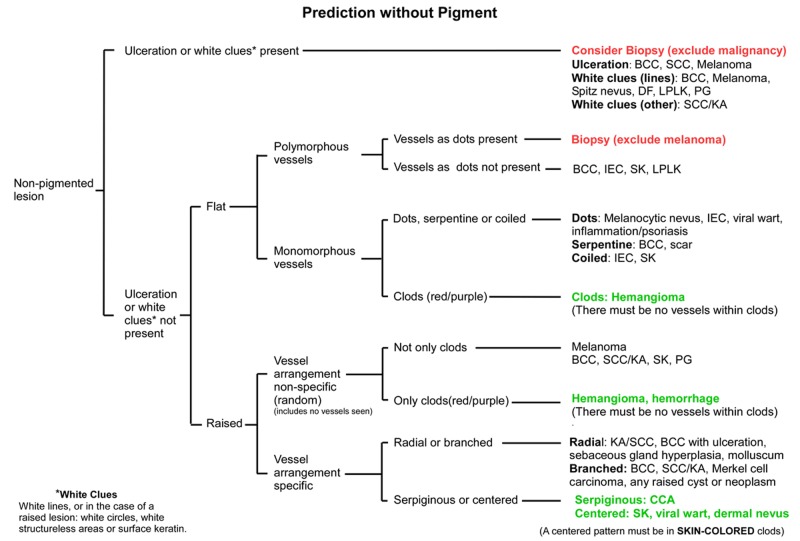
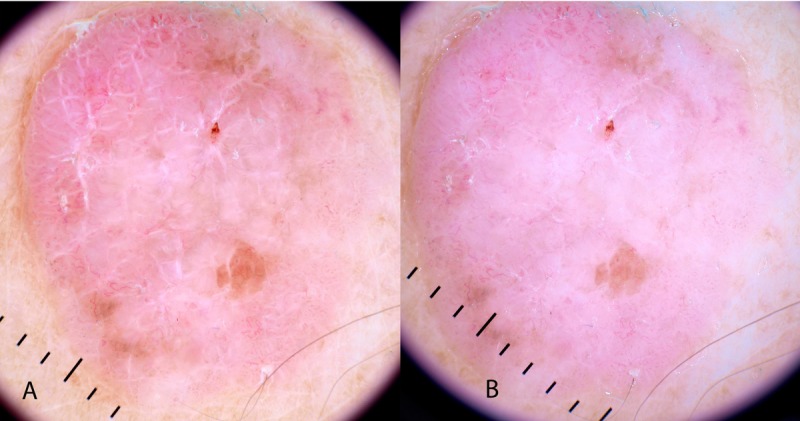
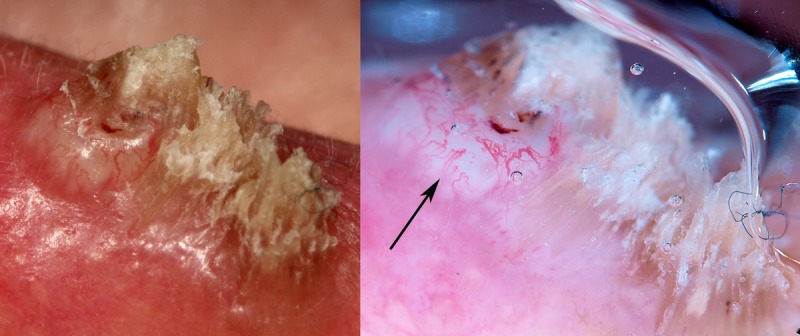
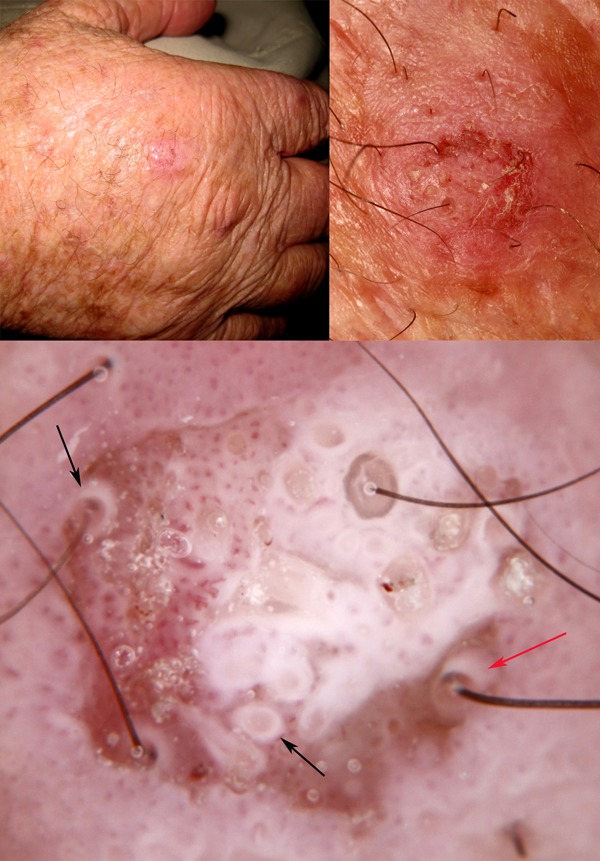
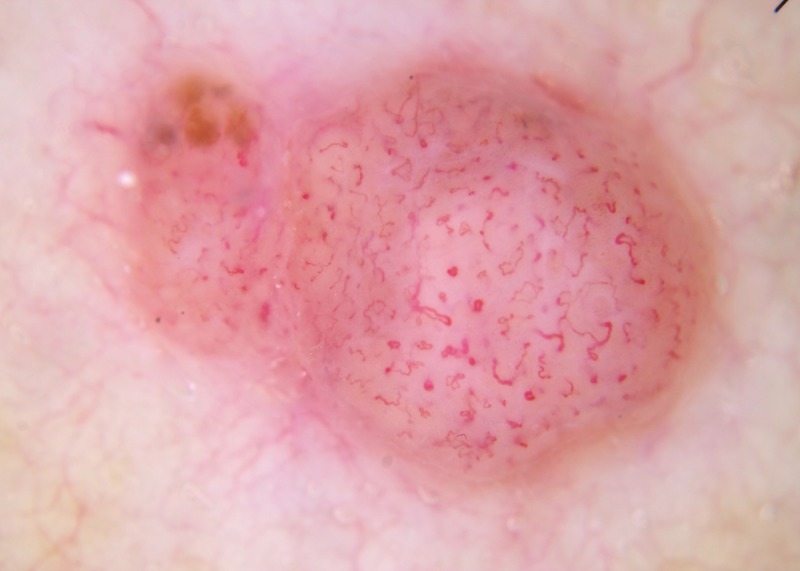
While there are several published comprehensive stepwise algorithmic methods for diagnosing pigmented skin malignancy, only limited material has been published for the stepwise assessment of non-pigmented lesions. We present a method based on pattern analysis, with a stepwise assessment, first, for ulceration, second, for white clues (defined as white lines, or in the case of a raised lesion any of the keratin clues: dermatoscopic white circles, dermatoscopic white structureless areas or surface keratin), and third, if no ulceration or white clues are present, proceed to vessel pattern analysis. This is a novel method, and apart from the assessment of white clues in raised lesions, it has not been formally tested. The priority of keratin clues in raised lesions over vessel pattern analysis has, however, been verified. It is conceded that this method is less specific than methods which have clues of pigmented structures, and accepting these limitations, Prediction without Pigment is a decision algorithm intended to guide the clinician in the decision as to whether to perform a biopsy rather than consistently leading to a specific diagnosis. Reaching a more specific diagnosis at the end of our flowchart can be achieved by weighing of clues both clinical and dermatoscopic, and that ability can be expected to improve with both knowledge and experience, but no diagnostic method, including this one, can be 100% sensitive in diagnosing malignancy, in particular, melanoma. Taking these limitations into account, any non-pigmented lesion, regardless of pattern analysis, which is raised and firm (nodular) and for which a confident, specific benign diagnosis cannot be made, should be excised to exclude the nodular variant of amelanotic melanoma.
虽然已经有几个发表的用于诊断色素性皮肤恶性肿瘤的全面逐步算法方法,但只有有限的材料被发表用于逐步评估非色素病变。我们提出了一种基于模式分析的方法,首先进行溃疡评估,其次是白色线索(定义为白线,或者在隆起病变的情况下,任何角化线索:皮肤镜下的白色圆圈、皮肤镜下无结构的白色区域或表面角化),如果没有溃疡或白色线索,则进行血管模式分析。这是一种新的方法,除了评估隆起病变中的白色线索外,它尚未经过正式测试。然而,角化线索在隆起病变中的优先级已经得到了验证。需要承认的是,与具有色素结构线索的方法相比,这种方法的特异性较低,在接受这些局限性的前提下,无色素预测是一种决策算法,旨在指导临床医生决定是否进行活检,而不是始终导致特定的诊断。通过对临床和皮肤镜下的线索进行权衡,可以在我们的流程图的最后达到更具体的诊断,并且随着知识和经验的积累,这种能力有望提高,但没有任何诊断方法,包括这种方法,能够 100%敏感地诊断恶性肿瘤,特别是黑色素瘤。考虑到这些局限性,任何非色素性病变,无论模式分析如何,如果是隆起且坚硬(结节状),并且无法做出明确的良性诊断,都应切除以排除无色素性黑素瘤的结节变体。