Cai Qiangjun, Mukku Venkata K, Ahmad Masood
Department of Cardiology, McFarland Clinic, 1215 Duff Avenue, Ames, IA 50010.
Curr Cardiol Rev. 2013 Nov;9(4):331-9. doi: 10.2174/1573403x10666140214122234.
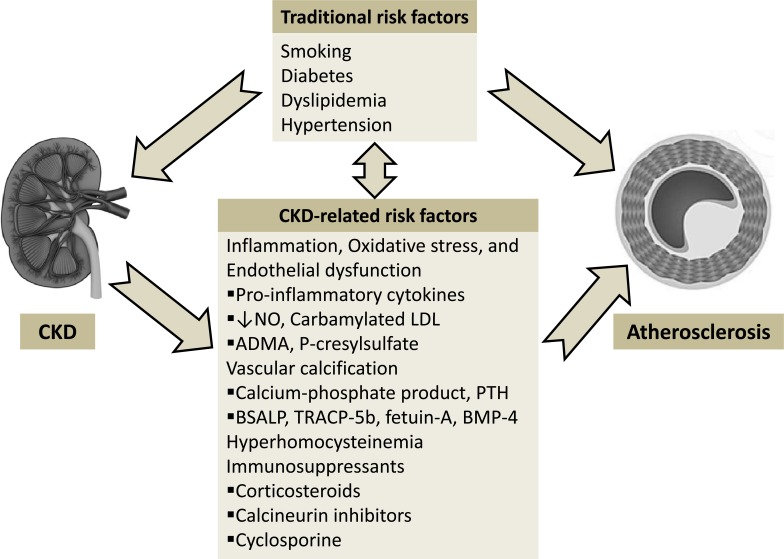
Chronic kidney disease (CKD) is an independent risk factor for coronary artery disease (CAD). Coronary artery disease is the leading cause of morbidity and mortality in patients with CKD. The outcomes of CAD are poorer in patients with CKD. In addition to traditional risk factors, several uremia-related risk factors such as inflammation, oxidative stress, endothelial dysfunction, coronary artery calcification, hyperhomocysteinemia, and immunosuppressants have been associated with accelerated atherosclerosis. A number of uremia-related biomarkers are identified as predictors of cardiac outcomes in CKD patients. The symptoms of CAD may not be typical in patients with CKD. Both dobutamine stress echocardiography and radionuclide myocardial perfusion imaging have moderate sensitivity and specificity in detecting obstructive CAD in CKD patients. Invasive coronary angiography carries a risk of contrast nephropathy in patients with advanced CKD. It should be reserved for those patients with a high risk for CAD and those who would benefit from revascularization. Guideline-recommended therapies are, in general, underutilized in renal patients. Medical therapy should be considered the initial strategy for clinically stable CAD. The effects of statins in patients with advanced CKD have been neutral despite a lipid-lowering effect. Compared to non-CKD population, percutaneous coronary intervention (PCI) is associated with higher procedure complications, restenosis, and future cardiac events even in the drug-eluting stent era in patients with CKD. Compared with PCI, coronary artery bypass grafting (CABG) reduces repeat revascularizations but is associated with significant perioperative morbidity and mortality. Screening for CAD is an important part of preoperative evaluation for kidney transplant candidates.
慢性肾脏病(CKD)是冠状动脉疾病(CAD)的独立危险因素。冠状动脉疾病是CKD患者发病和死亡的主要原因。CKD患者的CAD预后较差。除传统危险因素外,一些与尿毒症相关的危险因素,如炎症、氧化应激、内皮功能障碍、冠状动脉钙化、高同型半胱氨酸血症和免疫抑制剂,都与动脉粥样硬化加速有关。许多与尿毒症相关的生物标志物被确定为CKD患者心脏预后的预测指标。CAD的症状在CKD患者中可能不典型。多巴酚丁胺负荷超声心动图和放射性核素心肌灌注成像在检测CKD患者的阻塞性CAD方面具有中等的敏感性和特异性。有创冠状动脉造影在晚期CKD患者中有发生造影剂肾病的风险。它应仅用于CAD高危患者以及那些将从血运重建中获益的患者。一般来说,指南推荐的治疗方法在肾病患者中未得到充分利用。药物治疗应被视为临床稳定的CAD患者的初始策略。尽管他汀类药物有降脂作用,但在晚期CKD患者中其效果呈中性。与非CKD人群相比,即使在药物洗脱支架时代,经皮冠状动脉介入治疗(PCI)在CKD患者中也与更高的手术并发症、再狭窄和未来心脏事件相关。与PCI相比,冠状动脉旁路移植术(CABG)可减少再次血运重建,但与显著的围手术期发病率和死亡率相关。CAD筛查是肾移植候选者术前评估的重要组成部分。