Van Geertruyden J-P
Unit of International Health, University of Antwerp, Antwerp, Belgium.
Clin Microbiol Infect. 2014 Apr;20(4):278-85. doi: 10.1111/1469-0691.12597.
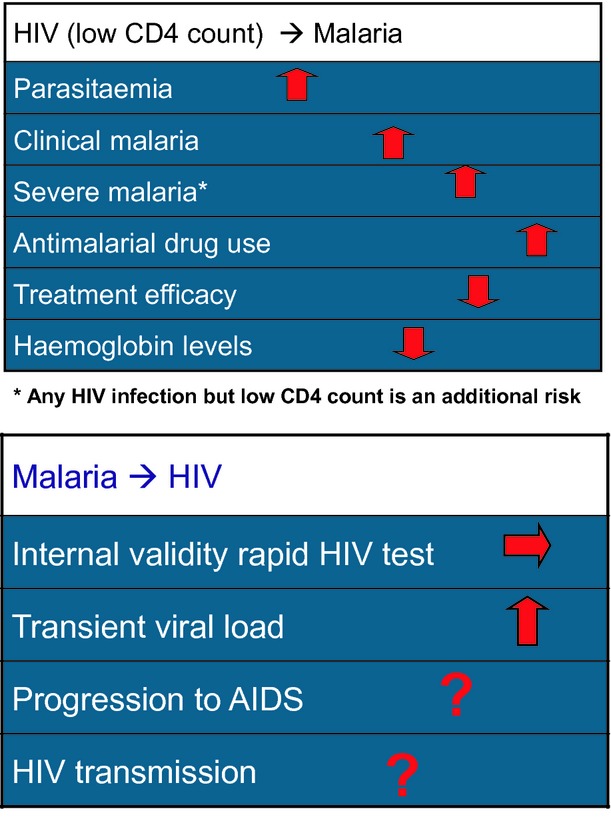
Possible pathophysiological, clinical and epidemiological interactions between human immunodeficiency virus (HIV) and tropical pathogens, especially malaria parasites, constitute a concern in tropical areas. Two decades of research have shown that HIV-related immunosuppression is correlated with increased malaria infection, burden, and treatment failure, and with complicated malaria, irrespective of immune status. The recent role out of antiretroviral therapies and new antimalarials, such as artemisinin combination therapies, raise additional concerns regarding possible synergistic and antagonistic effects on efficacy and toxicity. Co-trimoxazole, which is used to prevent opportunistic infections, has been shown to have strong antimalarial prophylactic properties, despite its long-term use and increasing antifolate resistance. The administration of efavirenz, a non-nucleoside reverse transcriptase inhibitor, with amodiaquine-artesunate has been associated with increased toxicity. Recent in vivo observations have confirmed that protease inhibitors have strong antimalarial properties. Ritonavir-boosted lopinavir and artemether-lumefantrine have a synergistic effect in terms of improved malaria treatment outcomes, with no apparent increase in the risk of toxicity. Overall, for the prevention and treatment of malaria in HIV-infected populations, the current standard of care is similar to that in non-HIV-infected populations. The available data show that the wider use of insecticide-treated bed-nets, co-trimoxazole prophylaxis and antiretroviral therapy might substantially reduce the morbidity of malaria in HIV-infected patients. These observations show that those accessing care for HIV infection are now, paradoxically, well protected from malaria. These findings therefore highlight the need for confirmatory diagnosis of malaria in HIV-infected individuals receiving these interventions, and the provision of different artemisinin-based combination therapies to treat malaria only when the diagnosis is confirmed.
人类免疫缺陷病毒(HIV)与热带病原体尤其是疟原虫之间可能存在的病理生理、临床及流行病学相互作用,是热带地区备受关注的问题。二十年的研究表明,无论免疫状态如何,HIV相关的免疫抑制都与疟疾感染增加、负担加重、治疗失败以及复杂型疟疾相关。近期抗逆转录病毒疗法及新型抗疟药(如青蒿素联合疗法)的应用,引发了人们对其在疗效和毒性方面可能存在的协同及拮抗作用的更多担忧。用于预防机会性感染的复方新诺明,尽管长期使用且耐叶酸耐药性不断增加,但已被证明具有强大的抗疟预防特性。非核苷类逆转录酶抑制剂依非韦伦与阿莫地喹-青蒿琥酯联合使用时,毒性有所增加。近期的体内观察证实蛋白酶抑制剂具有强大的抗疟特性。利托那韦增强的洛匹那韦与蒿甲醚-本芴醇在改善疟疾治疗效果方面具有协同作用,且毒性风险无明显增加。总体而言,对于HIV感染人群中疟疾的预防和治疗,目前的标准治疗方案与非HIV感染人群相似。现有数据表明,更广泛地使用经杀虫剂处理的蚊帐、复方新诺明预防及抗逆转录病毒疗法,可能会大幅降低HIV感染患者的疟疾发病率。这些观察结果表明,那些接受HIV感染治疗的人现在反而能很好地预防疟疾。因此,这些发现凸显了对接受这些干预措施的HIV感染个体进行疟疾确诊诊断的必要性,以及仅在确诊后提供不同的青蒿素类联合疗法来治疗疟疾的必要性。