Infectious Diseases Institute, Makerere University, Kampala, Uganda.
J Antimicrob Chemother. 2012 Sep;67(9):2213-21. doi: 10.1093/jac/dks207. Epub 2012 Jun 11.
Co-administration of artemether/lumefantrine with antiretroviral therapy has potential for pharmacokinetic drug interactions. We investigated drug-drug interactions between artemether/lumefantrine and efavirenz or nevirapine.
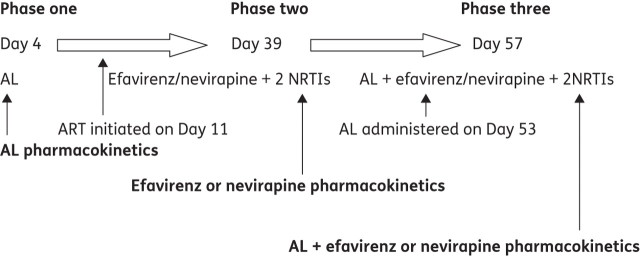
We performed a cross-over study in which HIV-infected adults received standard six-dose artemether/lumefantrine 80/480 mg before and at efavirenz or nevirapine steady state. Artemether, dihydroartemisinin, lumefantrine, efavirenz and nevirapine plasma concentrations were measured and compared.
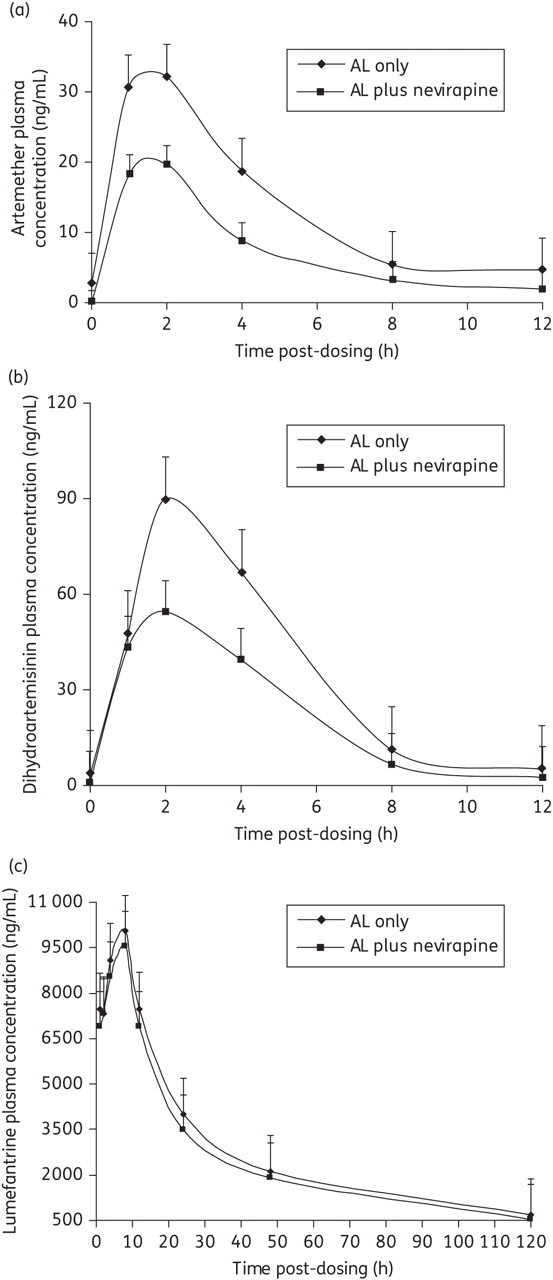
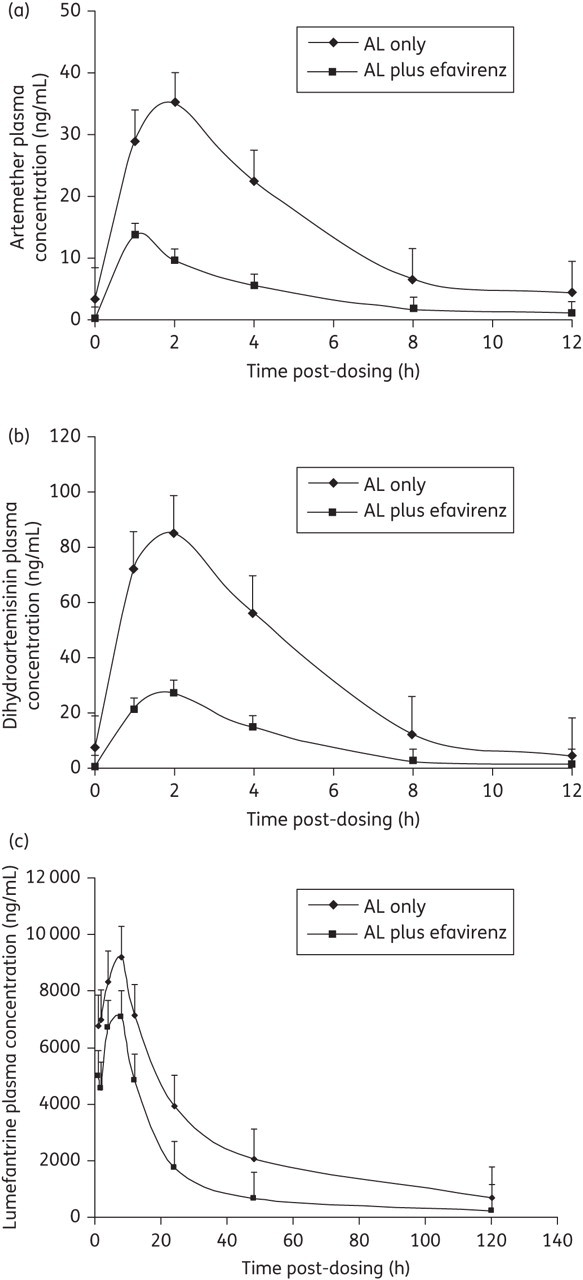
Efavirenz significantly reduced artemether maximum concentration (C(max)) and plasma AUC (median 29 versus 12 ng/mL, P < 0.01, and 119 versus 25 ng · h/mL, P < 0.01), dihydroartemisinin C(max) and AUC (median 120 versus 26 ng/mL, P < 0.01, and 341 versus 84 ng · h/mL, P < 0.01), and lumefantrine C(max) and AUC (median 8737 versus 6331 ng/mL, P = 0.03, and 280 370 versus 124 381 ng · h/mL, P < 0.01). Nevirapine significantly reduced artemether C(max) and AUC (median 28 versus 11 ng/mL, P < 0.01, and 123 versus 34 ng · h/mL, P < 0.01) and dihydroartemisinin C(max) and AUC (median 107 versus 59 ng/mL, P < 0.01, and 364 versus 228 ng · h/mL, P < 0.01). Lumefantrine C(max) and AUC were non-significantly reduced by nevirapine. Artemether/lumefantrine reduced nevirapine C(max) and AUC (median 8620 versus 4958 ng/mL, P < 0.01, and 66 329 versus 35 728 ng · h/mL, P < 0.01), but did not affect efavirenz exposure.
Co-administration of artemether/lumefantrine with efavirenz or nevirapine resulted in a reduction in artemether, dihydroartemisinin, lumefantrine and nevirapine exposure. These drug interactions may increase the risk of malaria treatment failure and development of resistance to artemether/lumefantrine and nevirapine. Clinical data from population pharmacokinetic and pharmacodynamic trials evaluating the impact of these drug interactions are urgently needed.
青蒿琥酯/咯萘啶与抗逆转录病毒疗法联合应用具有潜在的药代动力学药物相互作用。我们研究了青蒿琥酯/咯萘啶与依非韦伦或奈韦拉平之间的药物-药物相互作用。
我们进行了一项交叉研究,其中感染 HIV 的成年人在依非韦伦或奈韦拉平稳态时接受了标准的六剂青蒿琥酯/咯萘啶 80/480mg。测量并比较了青蒿琥酯、双氢青蒿素、咯萘啶、依非韦伦和奈韦拉平的血浆浓度。
依非韦伦显著降低了青蒿琥酯的最大浓度(C(max))和血浆 AUC(中位数 29 与 12ng/ml,P<0.01 和 119 与 25ng·h/ml,P<0.01)、双氢青蒿素 C(max)和 AUC(中位数 120 与 26ng/ml,P<0.01 和 341 与 84ng·h/ml,P<0.01),以及咯萘啶 C(max)和 AUC(中位数 8737 与 6331ng/ml,P=0.03 和 280370 与 124381ng·h/ml,P<0.01)。奈韦拉平显著降低了青蒿琥酯的 C(max)和 AUC(中位数 28 与 11ng/ml,P<0.01 和 123 与 34ng·h/ml,P<0.01)和双氢青蒿素的 C(max)和 AUC(中位数 107 与 59ng/ml,P<0.01 和 364 与 228ng·h/ml,P<0.01)。奈韦拉平对咯萘啶的 C(max)和 AUC 没有显著降低。青蒿琥酯/咯萘啶降低了奈韦拉平的 C(max)和 AUC(中位数 8620 与 4958ng/ml,P<0.01 和 66329 与 35728ng·h/ml,P<0.01),但不影响依非韦伦的暴露量。
青蒿琥酯/咯萘啶与依非韦伦或奈韦拉平联合使用导致青蒿琥酯、双氢青蒿素、咯萘啶和奈韦拉平的暴露量减少。这些药物相互作用可能增加疟疾治疗失败和青蒿琥酯/咯萘啶和奈韦拉平耐药的风险。急需评估这些药物相互作用影响的群体药代动力学和药效学临床试验的临床数据。