Tilbrook H E, Hewitt C E, Aplin J D, Semlyen A, Trewhela A, Watt I, Torgerson D J
York Trials Unit, Department of Health Sciences, University of York, York, UK.
York Trials Unit, Department of Health Sciences, University of York, York, UK.
Physiotherapy. 2014 Sep;100(3):256-62. doi: 10.1016/j.physio.2013.10.001. Epub 2013 Dec 4.
Methodological study nested within a multicentre randomised controlled trial (RCT) of yoga plus usual general practitioner (GP) care vs usual GP care for chronic low back pain.
To explore the treatment effects of non-compliance using three approaches in an RCT evaluating yoga for low back pain.
A large multicentre RCT using intention-to-treat (ITT) analysis found that participants with chronic low back pain who were offered a 12-week progressive programme of yoga plus usual GP care had better back function than those offered usual GP care alone. However, ITT analysis can underestimate the effect of treatment in those who comply with treatment. As such, the data were analysed using other approaches to assess the problem of non-compliance. The main outcome measure was the self-reported Roland Morris Disability Questionnaire (RMDQ).
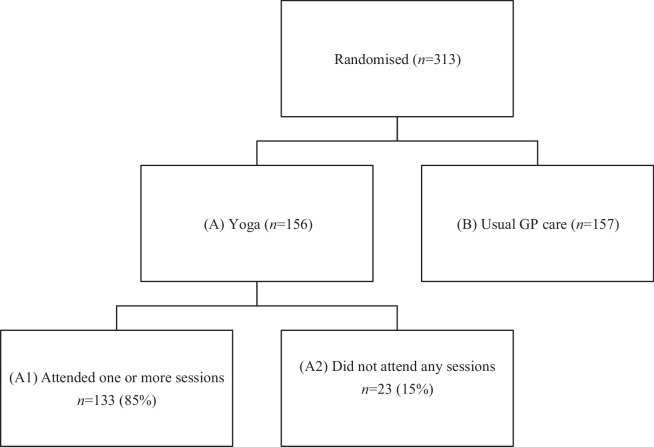
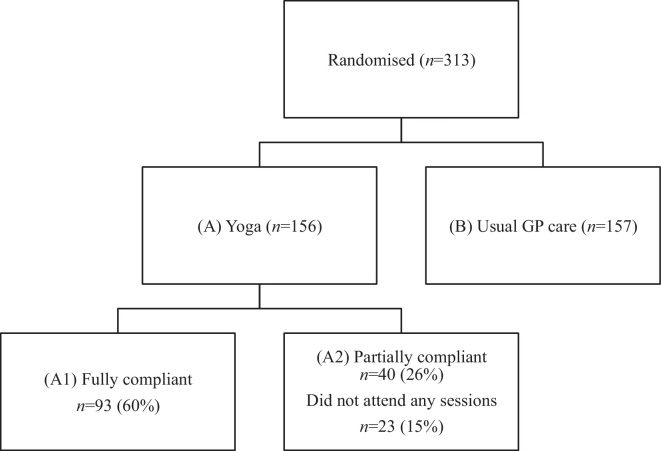
Complier average causal effect (CACE) analysis, per-protocol analysis and on-treatment analysis were conducted on the data of participants who were fully compliant, predefined as attendance of at least three of the first six sessions and at least three other sessions. The analysis was repeated for participants who had attended at least one yoga session (i.e. any compliance), which included participants who were fully compliant. Each approach was described, including strengths and weaknesses, and the results of the different approaches were compared with those of the ITT analysis.
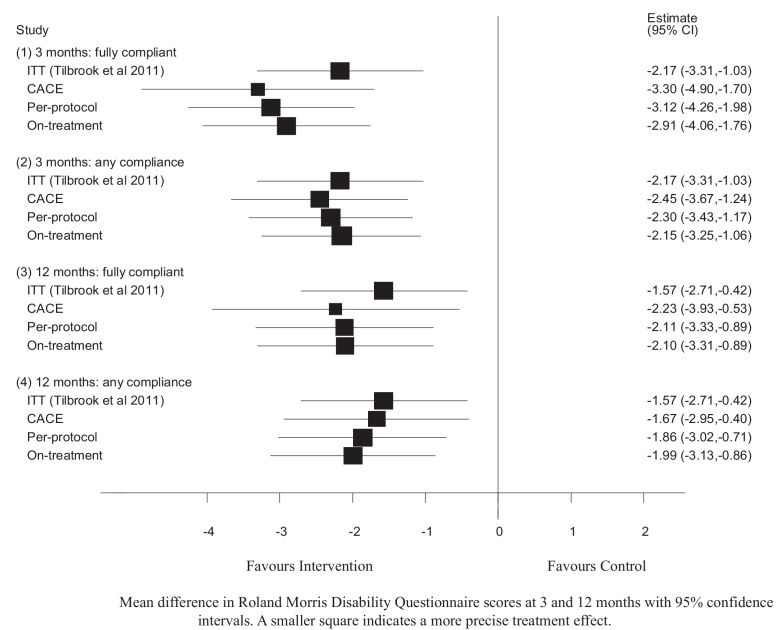
For the participants who were fully compliant (n=93, 60%), a larger beneficial treatment effect was seen using CACE analysis compared with per-protocol, on-treatment and ITT analyses at 3 and 12 months. The difference in mean change in RMDQ score between randomised groups was -3.30 [95% confidence interval (CI) -4.90 to -1.70, P<0.001] at 3 months and -2.23 (95% CI -3.93 to -0.53, P=0.010) at 12 months for CACE analysis, -3.12 (95% CI -4.26 to -1.98, P<0.001) at 3 months and -2.11 (95% CI -3.33 to -0.89, P=0.001) at 12 months for per-protocol analysis, and -2.91 (95% CI -4.06 to -1.76, P<0.001) at 3 months and -2.10 (95% CI -3.31 to -0.89, P=0.001) at 12 months for on-treatment analysis. For the participants who demonstrated any compliance (n=133, 85%), the results were generally consistent with the fully compliant group at 3 months, but the treatment effect was smaller. The difference in mean change in RMDQ score between randomised groups was -2.45 (95% CI -3.67 to -1.24) for CACE analysis, -2.30 (95% CI -3.43 to 1.17) for per-protocol analysis and -2.15 (95% CI -3.25 to -1.06) for on-treatment analysis, which was slightly less than that for ITT analysis. In contrast, at 12 months, per-protocol and on-treatment analyses showed a larger treatment effect compared with CACE and ITT analyses: per protocol analysis -1.86 (95% CI -3.02 to -0.71), on-treatment analysis -1.99 (95% CI -3.13 to -0.86) and CACE analysis -1.67 (95% CI -2.95 to -0.40).
ITT analysis estimated a slightly smaller treatment effect in participants who complied with treatment. When examining compliance, CACE analysis is more rigorous than per-protocol and on-treatment analyses. Using CACE analysis, the treatment effect was larger in participants who complied with treatment compared with participants who were allocated to treatment, and the difference between ITT and CACE analyses for the fully compliant group at 3 months was small but clinically important. Per-protocol and on-treatment analyses may produce unreliable estimates when the effect of treatment is small.
ISRCTN 81079604.
方法学研究,嵌套于一项多中心随机对照试验(RCT)中,该试验比较瑜伽联合普通全科医生(GP)常规护理与单纯GP常规护理对慢性下腰痛的疗效。
在一项评估瑜伽治疗下腰痛的RCT中,采用三种方法探讨不依从的治疗效果。
一项采用意向性分析(ITT)的大型多中心RCT发现,接受为期12周渐进式瑜伽课程联合普通GP常规护理的慢性下腰痛参与者,其背部功能优于仅接受普通GP常规护理的参与者。然而,ITT分析可能会低估依从治疗者的治疗效果。因此,采用其他方法对数据进行分析,以评估不依从问题。主要结局指标为自我报告的罗兰·莫里斯残疾问卷(RMDQ)。
对完全依从的参与者数据进行依从者平均因果效应(CACE)分析、符合方案分析和治疗中分析,完全依从定义为在前六次课程中至少参加三次,且在其他课程中至少参加三次。对至少参加过一次瑜伽课程(即任何程度的依从)的参与者重复进行分析,其中包括完全依从的参与者。描述了每种方法,包括优缺点,并将不同方法的结果与ITT分析结果进行比较。
对于完全依从的参与者(n = 93,60%),在3个月和12个月时,与符合方案分析、治疗中分析和ITT分析相比,CACE分析显示出更大的有益治疗效果。CACE分析中,随机分组组间RMDQ评分的平均变化差异在3个月时为-3.30 [95%置信区间(CI)-4.90至-1.70,P < 0.001],在12个月时为-2.23(95% CI -3.93至-0.53,P = 0.010);符合方案分析在3个月时为-3.12(95% CI -4.26至-1.98,P < 0.001),在12个月时为-2.11(95% CI -3.33至-0.89,P = 0.001);治疗中分析在3个月时为-2.91(95% CI -4.06至-1.76,P < 0.001),在12个月时为-2.10(95% CI -3.31至-0.89,P = 0.001)。对于有任何程度依从的参与者(n = 133,85%),结果在3个月时总体与完全依从组一致,但治疗效果较小。CACE分析中随机分组组间RMDQ评分的平均变化差异为-2.45(95% CI -3.67至-1.24),符合方案分析为-2.30(95% CI -3.43至1.17),治疗中分析为-2.15(95% CI -3.25至-1.06),略低于ITT分析。相比之下,在12个月时,符合方案分析和治疗中分析显示的治疗效果大于CACE分析和ITT分析:符合方案分析为-1.86(95% CI -3.02至-0.71),治疗中分析为-1.99(95% CI -3.13至-0.86),CACE分析为-1.67(95% CI -2.95至-0.40)。
ITT分析估计依从治疗的参与者治疗效果略小。在检查依从性时,CACE分析比符合方案分析和治疗中分析更严格。使用CACE分析,依从治疗的参与者治疗效果大于分配接受治疗的参与者,完全依从组在3个月时ITT分析与CACE分析的差异虽小但具有临床意义。当治疗效果较小时,符合方案分析和治疗中分析可能产生不可靠的估计。
ISRCTN 81079604。