Zhou Yi, Slack Rebecca, Jorgensen Jeffrey L, Wang Sa A, Rondon Gabriela, de Lima Marcos, Shpall Elizabeth, Popat Uday, Ciurea Stefan, Alousi Amin, Qazilbash Muzaffar, Hosing Chitra, O'Brien Susan, Thomas Deborah, Kantarjian Hagop, Medeiros L Jeffrey, Champlin Richard E, Kebriaei Partow
Department of Hematopathology, The University of Texas, M.D. Anderson Cancer Center, Houston, TX.
Department of Biostatistics, The University of Texas, M.D. Anderson Cancer Center, Houston, TX.
Clin Lymphoma Myeloma Leuk. 2014 Aug;14(4):319-26. doi: 10.1016/j.clml.2014.01.002. Epub 2014 Jan 15.
Allogeneic HSCT is highly effective for treating ALL. However, many ALL patients relapse after HSCT. There has been a continuing effort to improve identification of patients at high risk of relapse, with the goal of early intervention to improve outcome.
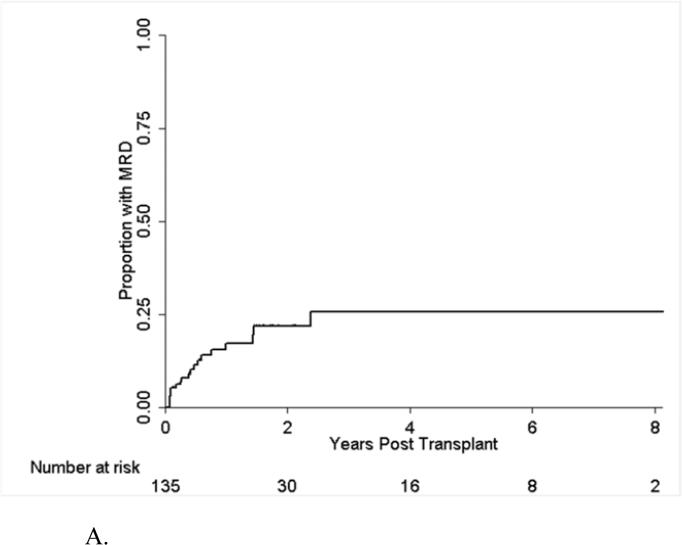
In this retrospective analysis, we examined the effect of MRD on the risk of hematologic relapse in 149 adult patients with ALL in morphologic remission undergoing allogeneic HSCT. MRD was assessed at the time of HSCT and after HSCT.
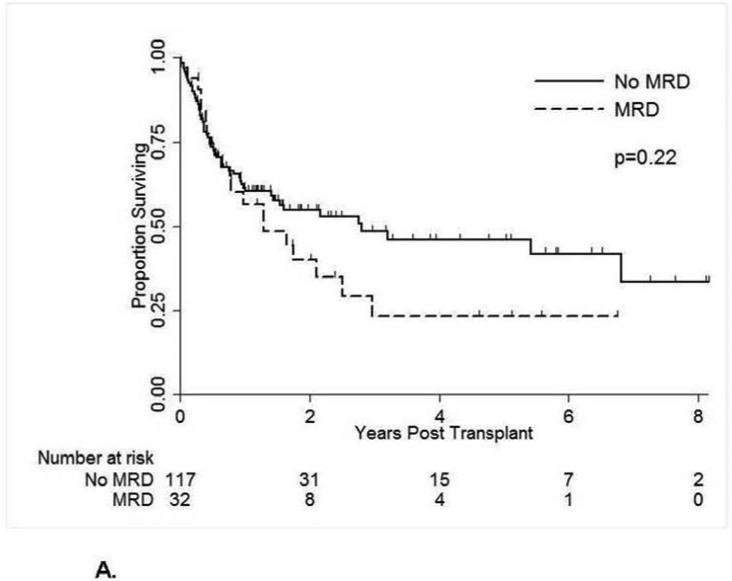
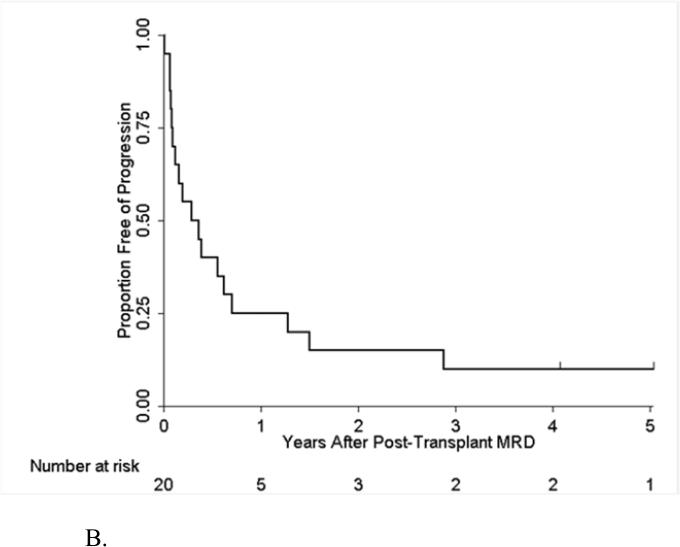
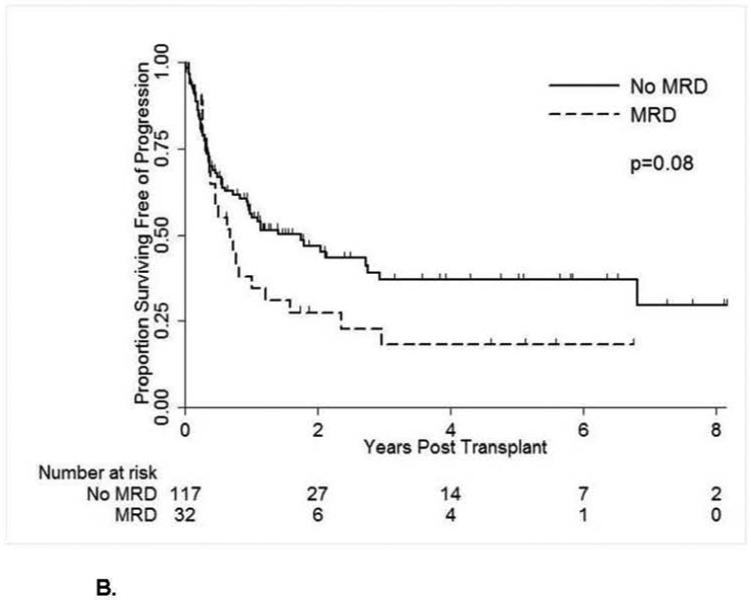
Patients with pretransplant MRD had a trend for shorter progression-free survival (PFS) at 2 years compared with patients without MRD, nearing statistical significance; 28% versus 47%, P = .08, on univariate analysis. This trend remained on multivariate analysis with better PFS in patients without MRD at the time of HSCT, hazard ratio (HR), 0.62 (95% confidence interval, 0.37-1.04); P = .07. Additionally, emergence of MRD after HSCT was a strong predictor for overt hematologic relapse (HR, 4; P < .001) with a median latency interval of 3.8 months.
These findings demonstrate the predictive value of monitoring for MRD around the time of transplant in adult patients with ALL.
异基因造血干细胞移植(HSCT)对治疗急性淋巴细胞白血病(ALL)非常有效。然而,许多ALL患者在HSCT后会复发。人们一直在不断努力改进对复发高危患者的识别,以期通过早期干预改善预后。
在这项回顾性分析中,我们研究了微小残留病(MRD)对149例形态学缓解的成年ALL患者接受异基因HSCT后血液学复发风险的影响。在HSCT时及HSCT后评估MRD。
与无MRD的患者相比,移植前有MRD的患者2年无进展生存期(PFS)有缩短趋势,接近统计学意义;单因素分析显示,分别为28%和47%,P = 0.08。多因素分析时该趋势依然存在,HSCT时无MRD的患者PFS更好,风险比(HR)为0.62(95%置信区间,0.37 - 1.04);P = 0.07。此外,HSCT后MRD的出现是明显血液学复发的有力预测指标(HR,4;P < 0.001),中位潜伏间隔为3.8个月。
这些发现证明了在成年ALL患者移植前后监测MRD的预测价值。