Casoni Gian Luca, Tomassetti Sara, Cavazza Alberto, Colby Thomas V, Dubini Alessandra, Ryu Jay H, Carretta Elisa, Tantalocco Paola, Piciucchi Sara, Ravaglia Claudia, Gurioli Christian, Romagnoli Micaela, Gurioli Carlo, Chilosi Marco, Poletti Venerino
Department of Diseases of the Thorax, G.B Morgagni Hospital, Forlì, Italy.
Department of Pathology, S. Maria Nuova Hospital-I.R.C.C.S, Reggio Emilia, Italy.
PLoS One. 2014 Feb 28;9(2):e86716. doi: 10.1371/journal.pone.0086716. eCollection 2014.
Histology is a key element for the multidisciplinary diagnosis of fibrotic diffuse parenchymal lung diseases (f-DPLD) when the clinical-radiological picture is nondiagnostic. Transbronchial lung cryobiopsy (TBLC) have been shown to be useful for obtaining large and well-preserved biopsies of lung parenchyma, but experience with TBLC in f-DPLD is limited.
To evaluate safety, feasibility and diagnostic yield of TBLC in f-DPLD.
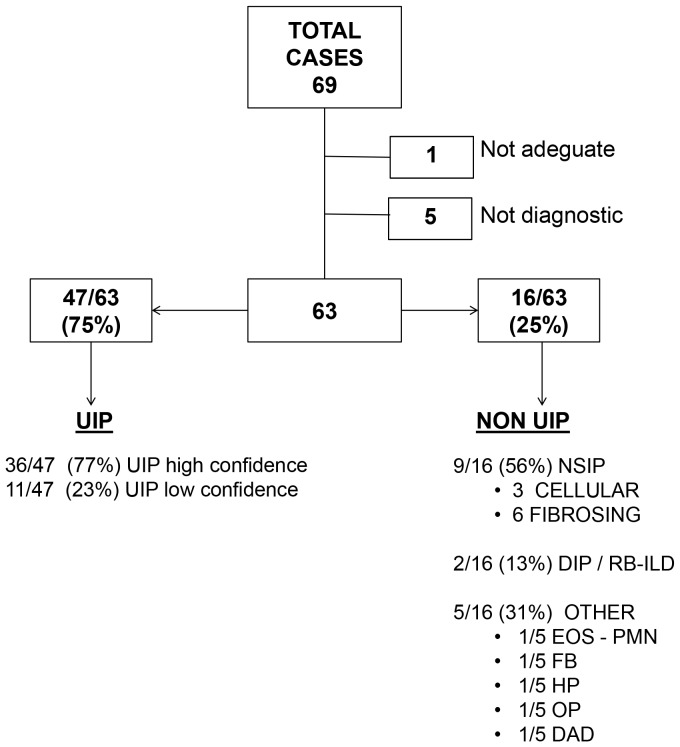
Prospective study of 69 cases of TBLC using flexible cryoprobe in the clinical-radiological setting of f-DPLD with nondiagnostic high resolution computed tomography (HRCT) features.
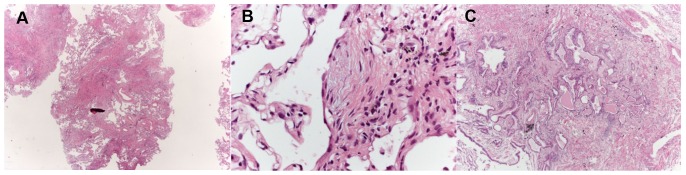
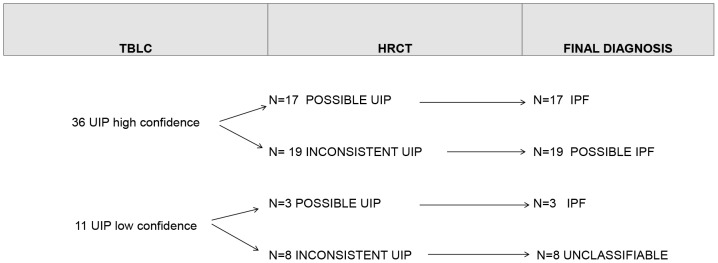
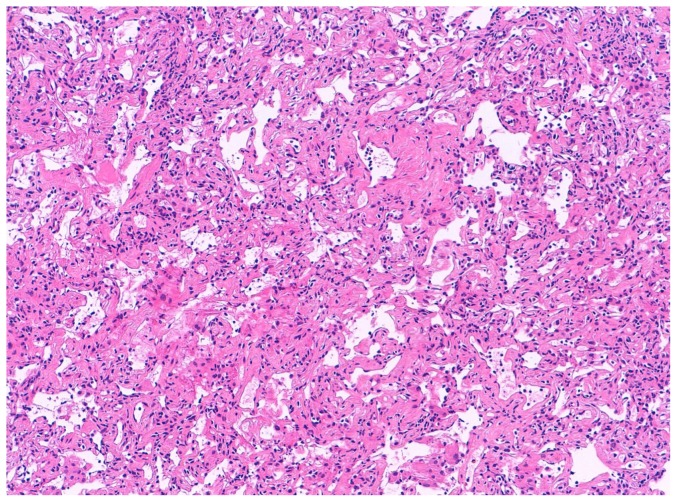
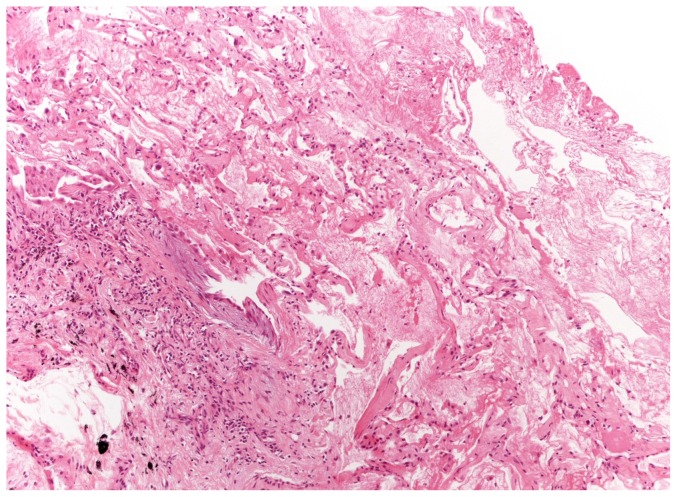
pneumothorax occurred in 19 patients (28%). One patient (1.4%) died of acute exacerbation. Feasibility: adequate cryobiopsies were obtained in 68 cases (99%). The median size of cryobiopsies was 43.11 mm(2) (range, 11.94-76.25). Diagnostic yield: among adequate TBLC the pathologists were confident ("high confidence") that histopathologic criteria sufficient to define a specific pattern in 52 patients (76%), including 36 of 47 with UIP (77%) and 9 nonspecific interstitial pneumonia (6 fibrosing and 3 cellular), 2 desquamative interstitial pneumonia/respiratory bronchiolitis-interstitial lung disease, 1 organizing pneumonia, 1 eosinophilic pneumonia, 1 diffuse alveolar damage, 1 hypersensitivity pneumonitis and 1 follicular bronchiolitis. In 11 diagnoses of UIP the pathologists were less confident ("low confidence"). Agreement between pathologists in the detection of UIP was very good with a Kappa coefficient of 0.83 (95% CI, 0.69-0.97). Using the current consensus guidelines for clinical-radiologic-pathologic correlation 32% (20/63) of cases were classified as Idiopathic Pulmonary Fibrosis (IPF), 30% (19/63) as possible IPF, 25% (16/63) as other f-DPLDs and 13% (8/63) were unclassifiable.
TBLC in the diagnosis of f-DPLD appears safe and feasible. TBLC has a good diagnostic yield in the clinical-radiological setting of f-DPLD without diagnostic HRCT features of usual interstitial pneumonia. Future studies should consider TBLC as a potential alternative to SLBx in f-DPLD.
当临床-放射学表现无法确诊时,组织学是纤维化弥漫性实质性肺疾病(f-DPLD)多学科诊断的关键要素。经支气管肺冷冻活检(TBLC)已被证明有助于获取大的且保存良好的肺实质活检组织,但TBLC在f-DPLD中的经验有限。
评估TBLC在f-DPLD中的安全性、可行性及诊断率。
对69例在f-DPLD临床-放射学背景下、高分辨率计算机断层扫描(HRCT)特征无法确诊时使用柔性冷冻探头进行TBLC的病例进行前瞻性研究。
19例患者(28%)发生气胸。1例患者(1.4%)死于急性加重。可行性:68例(99%)获得了足够的冷冻活检组织。冷冻活检组织的中位大小为43.11平方毫米(范围为11.94 - 76.25)。诊断率:在足够的TBLC病例中,病理学家有信心(“高信心”)认为组织病理学标准足以定义特定模式的有52例(76%),包括47例UIP中的36例(77%)以及9例非特异性间质性肺炎(6例纤维化型和3例细胞型)、2例脱屑性间质性肺炎/呼吸性细支气管炎-间质性肺疾病、1例机化性肺炎、1例嗜酸性肺炎、1例弥漫性肺泡损伤、1例过敏性肺炎和1例滤泡性细支气管炎。在11例UIP诊断中,病理学家信心较低(“低信心”)。病理学家在UIP检测方面的一致性非常好,Kappa系数为0.83(95%CI,0.69 - 0.97)。根据当前临床-放射学-病理学相关性的共识指南,32%(20/63)的病例被分类为特发性肺纤维化(IPF),30%(19/63)为可能的IPF,25%(16/63)为其他f-DPLD,13%(8/63)无法分类。
TBLC在f-DPLD诊断中似乎是安全可行的。在没有普通间质性肺炎诊断性HRCT特征的f-DPLD临床-放射学背景下,TBLC具有良好的诊断率。未来的研究应考虑将TBLC作为f-DPLD中外科肺活检(SLBx)的一种潜在替代方法。