Carroll Robert, Metcalfe Chris, Gunnell David
School of Social and Community Medicine, University of Bristol, Bristol, United Kingdom.
PLoS One. 2014 Feb 28;9(2):e89944. doi: 10.1371/journal.pone.0089944. eCollection 2014.
Non-fatal self-harm is one of the most frequent reasons for emergency hospital admission and the strongest risk factor for subsequent suicide. Repeat self-harm and suicide are key clinical outcomes of the hospital management of self-harm. We have undertaken a comprehensive review of the international literature on the incidence of fatal and non-fatal repeat self-harm and investigated factors influencing variation in these estimates as well as changes in the incidence of repeat self-harm and suicide over the last 30 years.
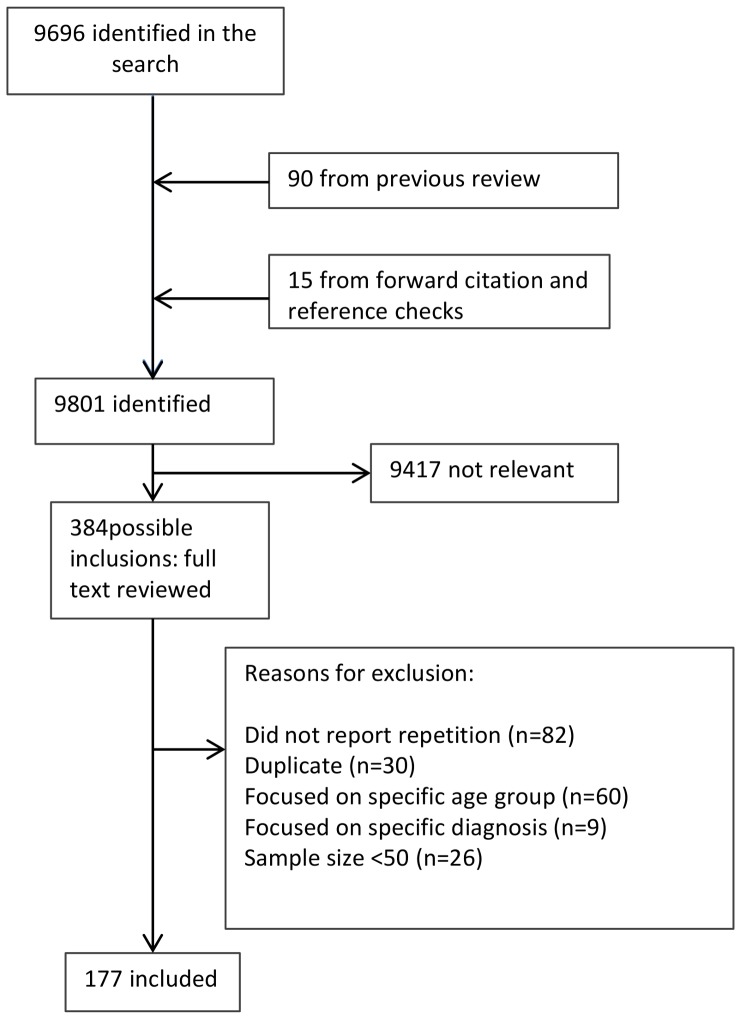
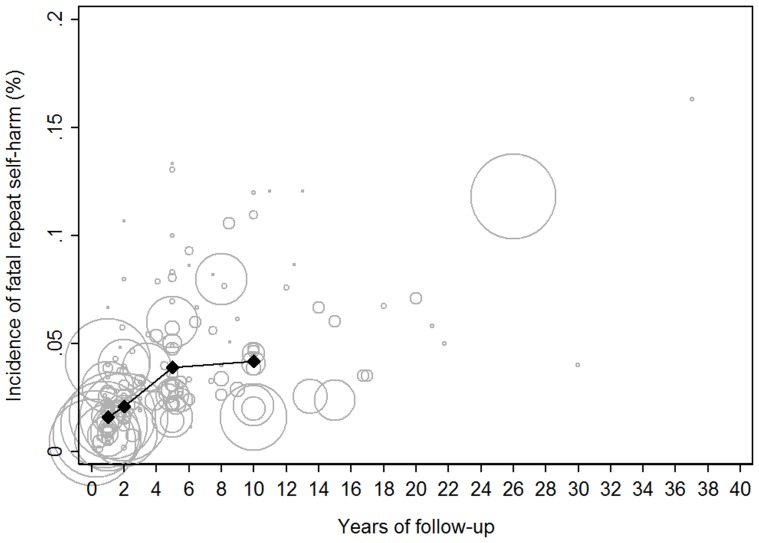
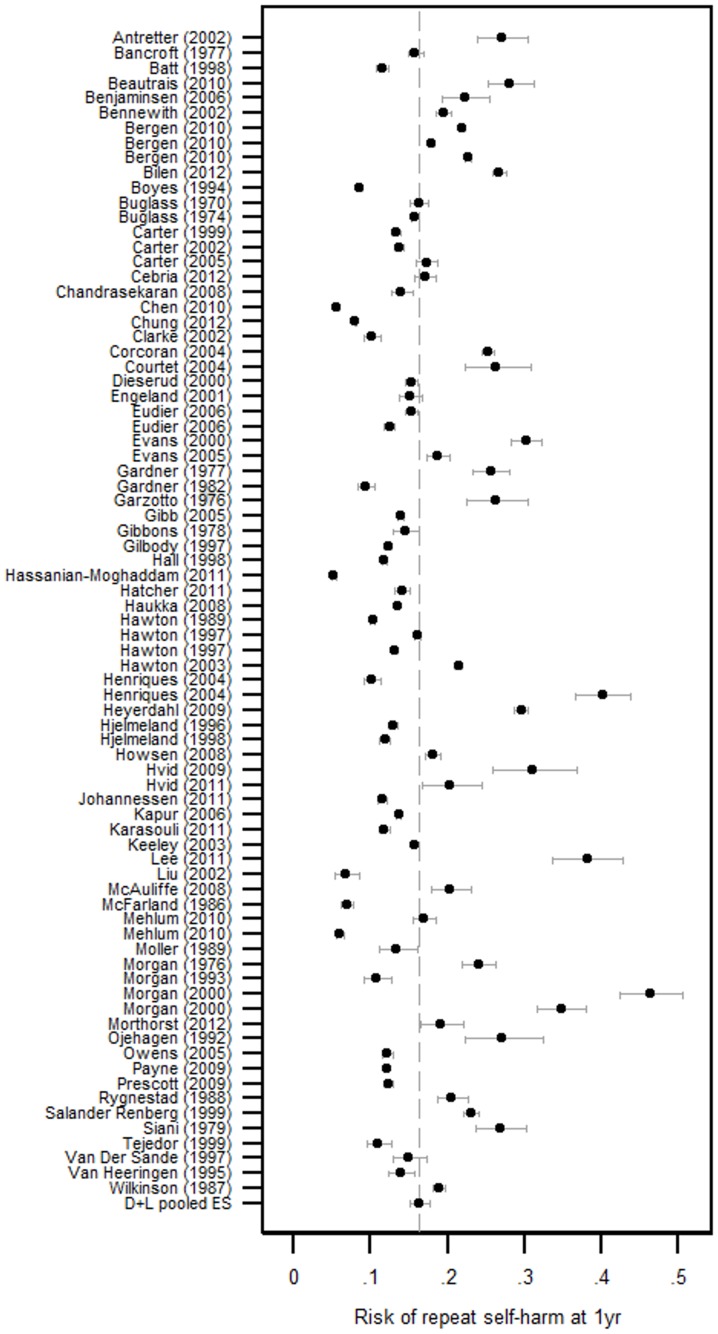
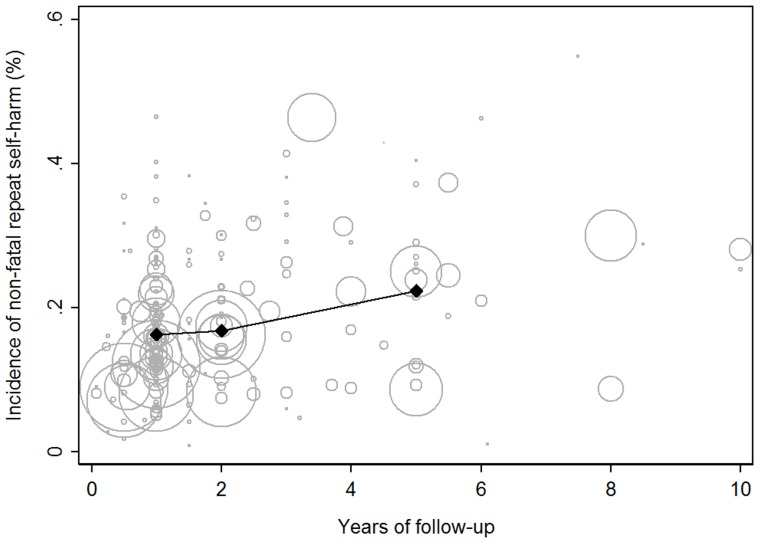
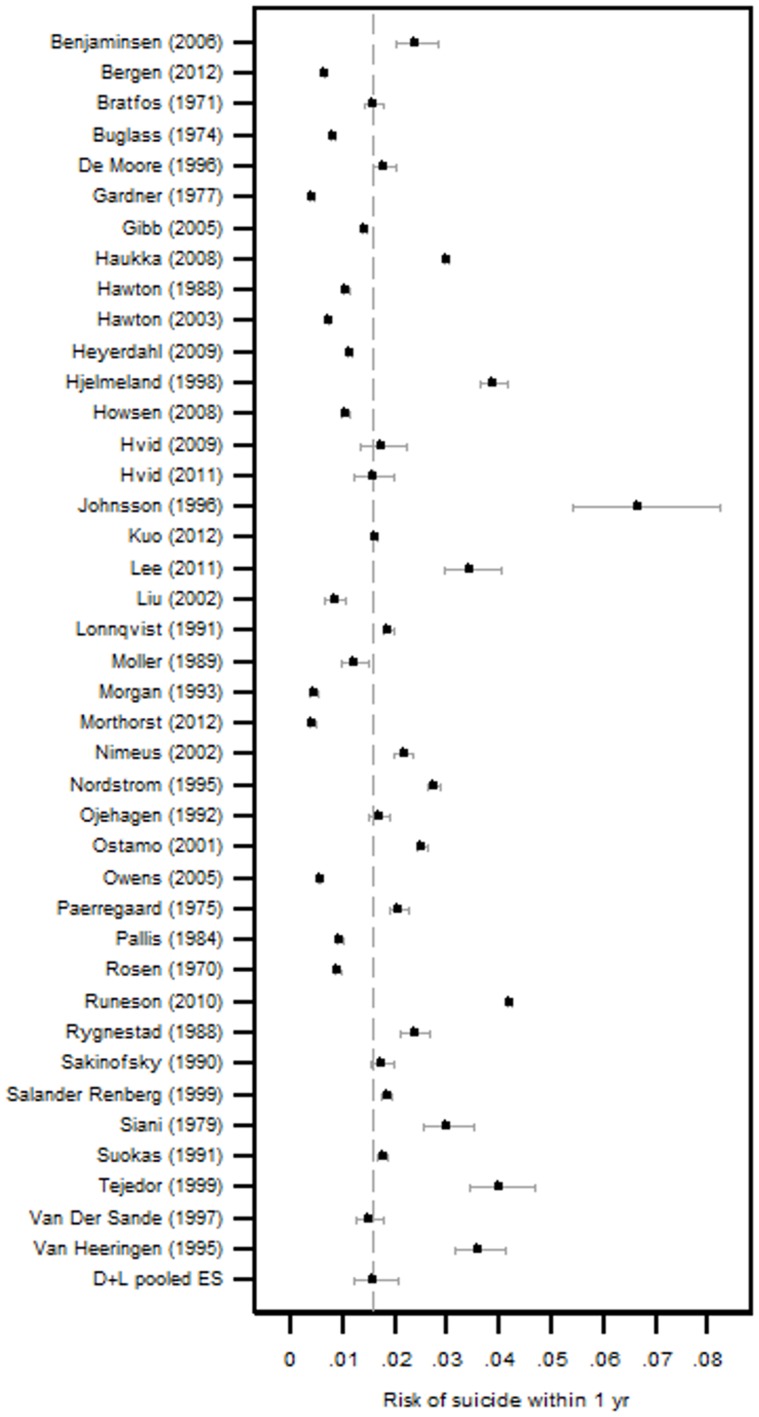
Medline, EMBASE, PsycINFO, Google Scholar, article reference lists and personal paper collections of the authors were searched for studies describing rates of fatal and non-fatal self-harm amongst people who presented to health care services for deliberate self-harm. Heterogeneity in pooled estimates of repeat self-harm incidence was investigated using stratified meta-analysis and meta-regression. The search identified 177 relevant papers. The risk of suicide in the 12 months after an index attempt was 1.6% (CI 1.2-2.4) and 3.9% (CI 3.2-4.8) after 5 years. The estimated 1 year rate of non-fatal repeat self-harm was 16.3% (CI 15.1-17.7). This proportion was considerably lower in Asian countries (10.0%, CI 7.3-13.6%) and varies between studies identifying repeat episodes using hospital admission data (13.7%, CI 12.3-15.3) and studies using patient report (21.9%, CI 14.3-32.2). There was no evidence that the incidence of repeat self-harm was lower in more recent (post 2000) studies compared to those from the 1980s and 1990s.
One in 25 patients presenting to hospital for self-harm will kill themselves in the next 5 years. The incidence of repeat self-harm and suicide in this population has not changed in over 10 years. Different methods of identifying repeat episodes of self-harm produce varying estimates of incidence and this heterogeneity should be considered when evaluating interventions aimed at reducing non-fatal repeat self-harm.
非致命性自我伤害是急诊入院最常见的原因之一,也是后续自杀最强的风险因素。重复性自我伤害和自杀是自我伤害医院管理的关键临床结果。我们对国际上关于致命性和非致命性重复性自我伤害发生率的文献进行了全面综述,并调查了影响这些估计值差异的因素,以及过去30年中重复性自我伤害和自杀发生率的变化。
检索了Medline、EMBASE、PsycINFO、谷歌学术、文章参考文献列表以及作者的个人论文集,以查找描述向医疗服务机构寻求蓄意自我伤害者中致命性和非致命性自我伤害发生率的研究。使用分层荟萃分析和荟萃回归研究重复性自我伤害发生率合并估计值的异质性。检索共识别出177篇相关论文。初次尝试后12个月内自杀风险为1.6%(95%置信区间1.2 - 2.4),5年后为3.9%(95%置信区间3.2 - 4.8)。估计非致命性重复性自我伤害的1年发生率为16.3%(95%置信区间15.1 - 17.7)。这一比例在亚洲国家显著较低(10.0%,95%置信区间7.3 - 13.6%),并且在使用医院入院数据识别重复发作的研究(13.7%,95%置信区间12.3 - 15.3)和使用患者报告的研究(21.9%,95%置信区间14.3 - 32.2)之间存在差异。没有证据表明与20世纪80年代和90年代的研究相比,近期(2000年后)研究中重复性自我伤害的发生率更低。
每25名因自我伤害入院的患者中就有1人会在未来5年内自杀。该人群中重复性自我伤害和自杀的发生率在10多年来没有变化。识别自我伤害重复发作的不同方法会产生不同的发生率估计值,在评估旨在减少非致命性重复性自我伤害的干预措施时应考虑这种异质性。