Yoon Vivienne, Heyliger Aliya, Maekawa Takashi, Sasano Hironobu, Carrick Kelley, Woodruff Stacey, Rabaglia Jennifer, Auchus Richard J, Ghayee Hans K
Department of Internal Medicine/Division of Endocrinology and Metabolism VA North Texas Health Care System and the University of Texas Southwestern Medical Center 5323 Harry Hines Boulevard, Dallas, Texas, 75390-8857 USA.
Department of Pathology Tohoku University School of Medicine and Hospital at Sendai Sendai Japan.
Endocrinol Diabetes Metab Case Rep. 2013;2013:130042. doi: 10.1530/EDM-13-0042. Epub 2013 Sep 23.
To recognize that benign adrenal adenomas can co-secrete excess aldosterone and cortisol, which can change clinical management.
We reviewed the clinical and histological features of an adrenal tumor co-secreting aldosterone and cortisol in a patient. Biochemical testing as well as postoperative immunohistochemistry was carried out on tissue samples for assessing enzymes involved in steroidogenesis.
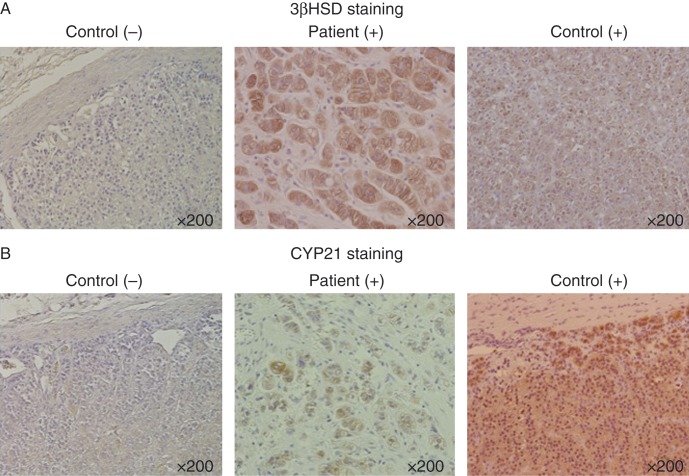
A patient presented with hypertension, hypokalemia, and symptoms related to hypercortisolism. The case demonstrated suppressed renin concentrations with an elevated aldosterone:renin ratio, abnormal dexamethasone suppression test results, and elevated midnight salivary cortisol concentrations. The patient had a right adrenal nodule with autonomous cortisol production and interval growth. Right adrenalectomy was carried out. Postoperatively, the patient tolerated the surgery, but he was placed on a short course of steroid replacement given a subnormal postoperative serum cortisol concentration. Long-term follow-up of the patient showed that his blood pressure and glucose levels had improved. Histopathology slides showed positive staining for 3β-hydroxysteroid dehydrogenase, 11β-hydroxylase, and 21 hydroxylase.
In addition to the clinical manifestations and laboratory values, the presence of these enzymes in this type of tumor provides support that the tumor in this patient was able to produce mineralocorticoids and glucocorticoids. The recognition of patients with a tumor that is co-secreting aldosterone and cortisol can affect decisions to treat with glucocorticoids perioperatively to avoid adrenal crisis.
Recognition of the presence of adrenal adenomas co-secreting mineralocorticoids and glucocorticoids.Consideration for perioperative and postoperative glucocorticoid use in the treatment of co-secreting adrenal adenomas.
认识到良性肾上腺腺瘤可同时分泌过量醛固酮和皮质醇,这会改变临床治疗方案。
我们回顾了一名肾上腺肿瘤同时分泌醛固酮和皮质醇患者的临床及组织学特征。对组织样本进行了生化检测及术后免疫组化,以评估参与类固醇生成的酶。
一名患者出现高血压、低钾血症及与皮质醇增多症相关的症状。该病例显示肾素浓度受抑制,醛固酮与肾素比值升高,地塞米松抑制试验结果异常,午夜唾液皮质醇浓度升高。患者右侧肾上腺有一个自主分泌皮质醇且有间隔性生长的结节。实施了右侧肾上腺切除术。术后,患者耐受手术,但因术后血清皮质醇浓度低于正常水平,接受了短期类固醇替代治疗。对该患者的长期随访显示其血压和血糖水平有所改善。组织病理学切片显示3β - 羟类固醇脱氢酶、11β - 羟化酶和21羟化酶呈阳性染色。
除临床表现和实验室检查结果外,这类肿瘤中这些酶的存在支持该患者的肿瘤能够产生盐皮质激素和糖皮质激素这一观点。识别出同时分泌醛固酮和皮质醇的肿瘤患者会影响围手术期使用糖皮质激素以避免肾上腺危象的治疗决策。
认识到存在同时分泌盐皮质激素和糖皮质激素的肾上腺腺瘤。在治疗同时分泌的肾上腺腺瘤时考虑围手术期和术后使用糖皮质激素。