Universidade Federal de São Paulo, Escola Paulista de Medicina, Departamento de Otorrinolaringologia e Cirurgia de Cabeça e Pescoço, São PauloSP, Brasil, Departamento de Otorrinolaringologia e Cirurgia de Cabeça e Pescoço, Universidade Federal de São Paulo / Escola Paulista de Medicina (UNIFESP/EPM), São Paulo, SP, Brasil.
Universidade Federal de São Paulo, Escola Paulista de Medicina, Departamento de Nefrologia, São PauloSP, Brasil, Departamento de Nefrologia, Universidade Federal de São Paulo / Escola Paulista de Medicina (UNIFESP/EPM), São Paulo, SP, Brasil.
Braz J Otorhinolaryngol. 2014 Jan-Feb;80(1):29-34. doi: 10.5935/1808-8694.20140008.
Hyperparathyroidism is an expected metabolic consequence of chronic kidney disease (CKD). Ectopic and/or supernumerary parathyroid glands (PT) may be the cause of surgical failure in patients undergoing total parathyroidectomy (PTX).
To define the locations of ectopic and supernumerary PT in patients with renal hyperparathyroidism and to correlate intraoperative findings with preoperative tests.
A retrospective study was conducted with 166 patients submitted to PTX. The location of PT during surgery was recorded and classified as eutopic or ectopic. The preoperative localizations of PT found by ultrasonography (USG) and Tc99m-Sestamibi scintigraphy (MIBI) were subsequently compared with intraoperative findings.
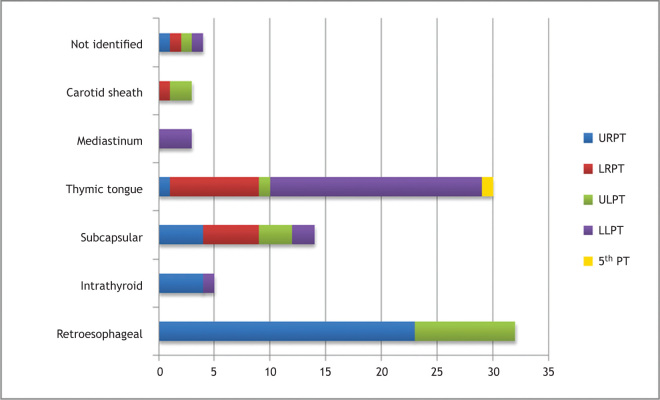
In the 166 patients studied, 664 PT were found. Five-hundred-seventy-seven (86.4%) glands were classified as eutopic and 91(13.6%) as ectopic. Eight supernumerary PT were found. The most common sites of ectopic PT were in the retroesophageal and thymic regions. Taken together, USG and MIBI did not identify 56 (61.5%) ectopic glands. MIBI was positive for 69,7% of all ectopic glands located in the mediastinal and thymic regions.
The presence of ectopic and supernumerary PT in patients with renal hyperparathyroidism is significant. Although preoperative imaging tests did not locate most of ectopic glands, MIBI may be important for identifying ectopic PT in the mediastinal and thymic regions.
甲状旁腺功能亢进症是慢性肾脏病(CKD)的预期代谢后果。异位和/或多余甲状旁腺(PT)可能是接受甲状旁腺全切除术(PTX)的患者手术失败的原因。
确定患有肾性甲状旁腺功能亢进症的患者中异位和多余 PT 的位置,并将术中发现与术前检查相关联。
对 166 例接受 PTX 的患者进行了回顾性研究。记录手术期间 PT 的位置,并将其分类为固有或异位。随后将超声(USG)和 Tc99m-Sestamibi 闪烁显像(MIBI)术前定位的 PT 与术中发现进行比较。
在研究的 166 例患者中,发现了 664 个 PT。577 个(86.4%)腺体被分类为固有,91 个(13.6%)为异位。发现 8 个多余的 PT。异位 PT 最常见的部位是食管后和胸腺区。超声和 MIBI 共未识别出 56 个(61.5%)异位腺体。位于纵隔和胸腺区的所有异位腺体中,MIBI 的阳性率为 69.7%。
在患有肾性甲状旁腺功能亢进症的患者中存在异位和多余的 PT 是很重要的。尽管术前影像学检查未定位出大多数异位腺体,但 MIBI 可能对识别纵隔和胸腺区的异位 PT 很重要。