Department of Transplant and Endocrine Surgery, Nagoya Daini Red Cross Hospital, Nagoya, Aichi, Japan.
PLoS One. 2021 Apr 1;16(4):e0248366. doi: 10.1371/journal.pone.0248366. eCollection 2021.
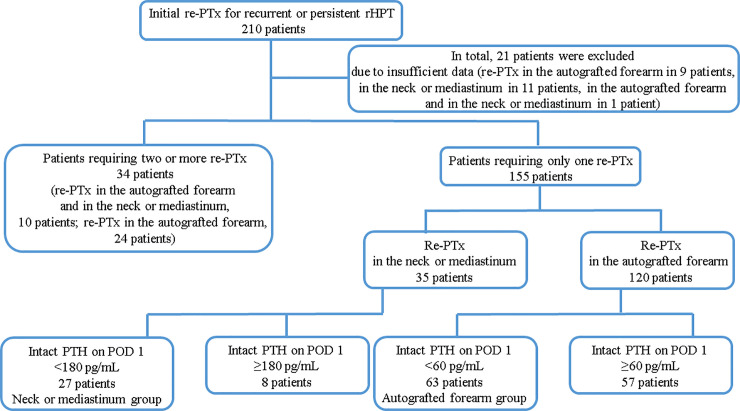
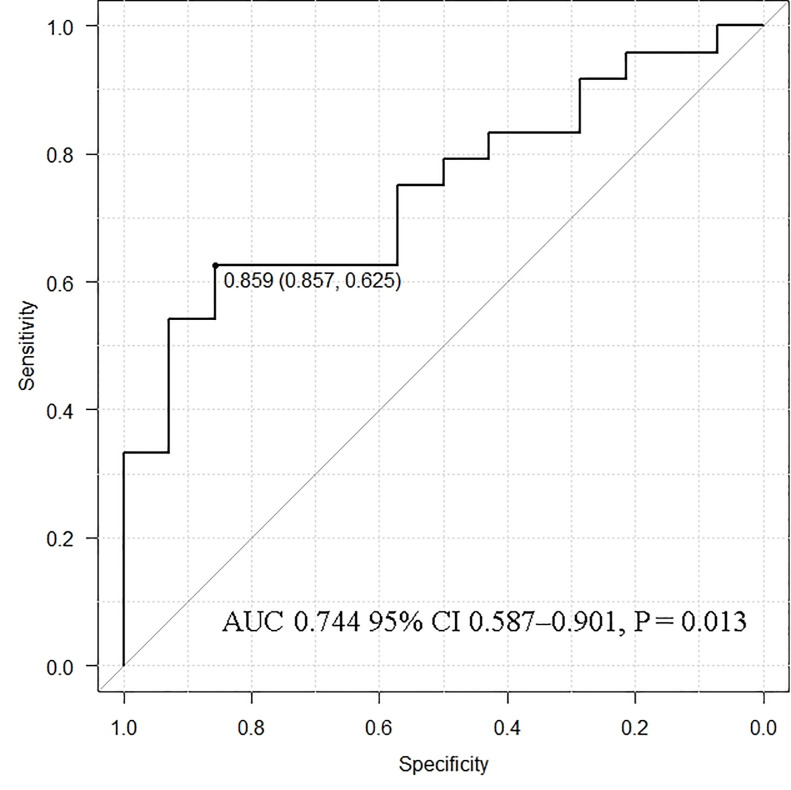
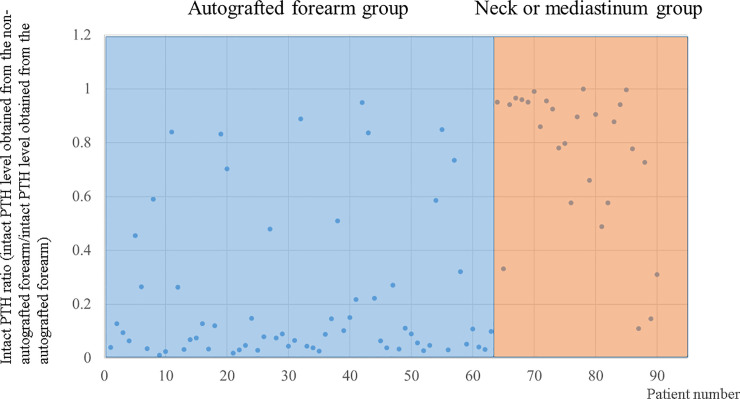
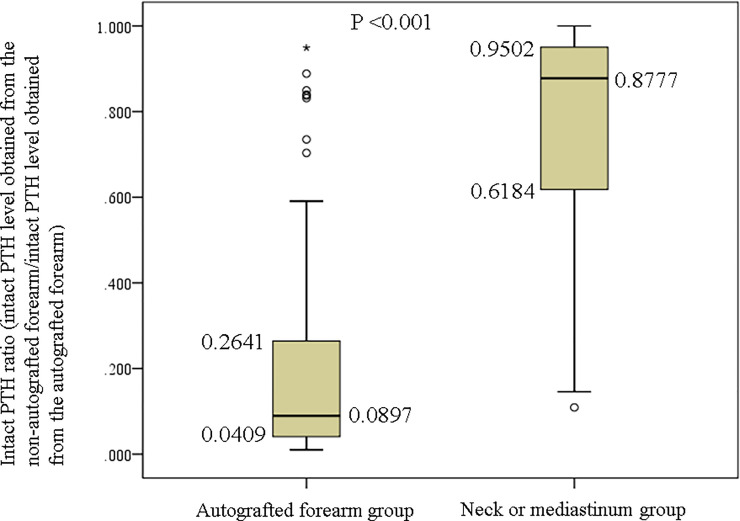
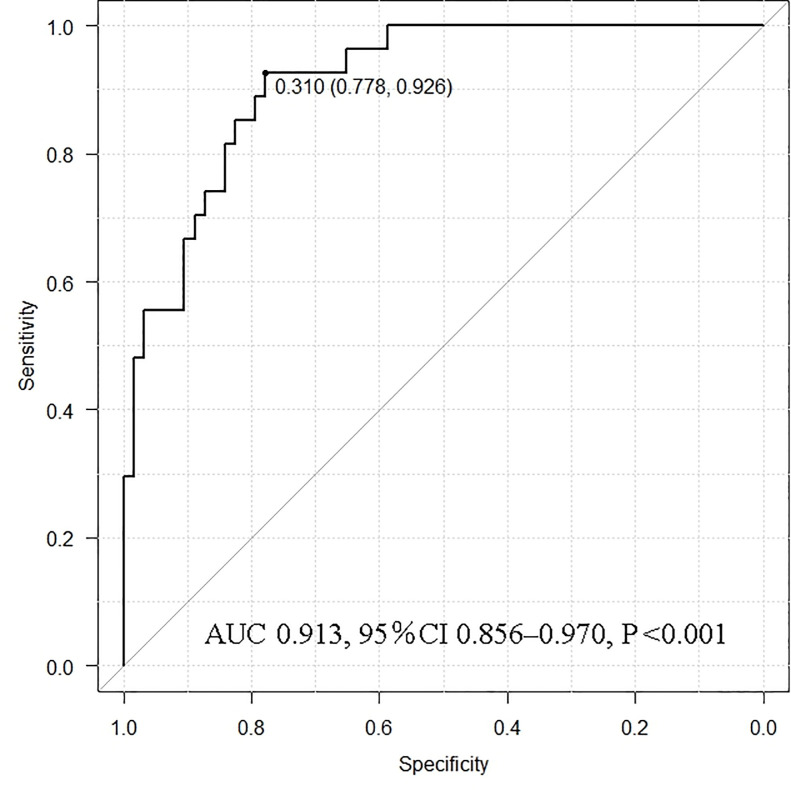
Persistent or recurrent renal hyperparathyroidism may occur after total parathyroidectomy and transcervical thymectomy with forearm autograft under continuous stimulation due to uremia. Parathyroid hormone (PTH) levels may reflect persistent or recurrent renal hyperparathyroidism because of the enlarged autografted parathyroid glands in the forearm or remnant parathyroid glands in the neck or mediastinum. Detailed imaging requires predictive localization of causative parathyroid glands. Casanova and simplified Casanova tests may be convenient. However, these methods require avascularization of the autografted forearm for >10 min with a tourniquet or Esmarch. The heavy pressure during avascularization can be incredibly painful and result in nerve damage. An easier method that minimizes the burden on patients in addition to predicting the localization of causative parathyroid glands was developed in this study. Ninety patients who underwent successful re-parathyroidectomy for persistent or recurrent renal hyperparathyroidism after parathyroidectomy between January 2000 and July 2019 were classified according to the localization of causative parathyroid glands (63 and 27 patients in the autografted forearm and the neck or mediastinum groups, respectively). Preoperatively, intact PTH levels were measured from bilateral forearm blood samples following a 5-min avascularization of the autografted forearm. Cutoff values of the intact PTH ratio (intact PTH level obtained from the non-autografted forearm before re-parathyroidectomy/intact PTH level obtained from the autografted forearm before re-parathyroidectomy) were investigated with receiver operating characteristic curves to localize the causative parathyroid glands. Intact PTH ratios of <0.310 with an area under the curve (AUC) of 0.913 (95% confidence interval [CI]: 0.856-0.970; P < 0.001) and >0.859 with an AUC 0.744 (95% CI: 0.587-0.901; P = 0.013) could predict causative parathyroid glands in the autografted forearm and the neck or mediastinum with diagnostic accuracies of 81.1% and 83.3%, respectively. Therefore, we propose that the intact PTH ratio is useful for predicting the localization of causative parathyroid glands for re-parathyroidectomy.
持续性或复发性肾性甲状旁腺功能亢进症可能发生在全甲状腺切除术后和颈前路胸腺切除术伴前臂自体移植后,原因是尿毒症持续刺激。甲状旁腺激素(PTH)水平可能反映持续性或复发性肾性甲状旁腺功能亢进症,因为前臂移植的甲状旁腺腺体增大或颈部或纵隔中的残余甲状旁腺腺体。详细的影像学需要对致病甲状旁腺进行预测性定位。卡索纳瓦和简化的卡索纳瓦试验可能很方便。然而,这些方法需要用止血带或埃斯马克勒使移植的前臂缺血化>10 分钟。缺血化期间的重压会非常痛苦,并导致神经损伤。本研究中开发了一种更简单的方法,除了预测致病甲状旁腺的定位外,还最大限度地减轻了患者的负担。2000 年 1 月至 2019 年 7 月期间,90 例因甲状旁腺切除术后持续性或复发性肾性甲状旁腺功能亢进症而行再次甲状旁腺切除术的患者,根据致病甲状旁腺的定位进行分类(分别为 63 例和 27 例在移植前臂和颈部或纵隔组)。术前,在缺血化 5 分钟后,从双侧前臂血样中测量完整的 PTH 水平。使用接收者操作特性曲线研究完整的 PTH 比值(在再次甲状旁腺切除术前取自非自体移植前臂的完整 PTH 水平/在再次甲状旁腺切除术前取自自体移植前臂的完整 PTH 水平)的截断值,以定位致病甲状旁腺。完整的 PTH 比值<0.310,曲线下面积(AUC)为 0.913(95%置信区间[CI]:0.856-0.970;P <0.001)和>0.859,AUC 为 0.744(95%CI:0.587-0.901;P=0.013)可以预测自体移植前臂和颈部或纵隔中的致病甲状旁腺,诊断准确率分别为 81.1%和 83.3%。因此,我们提出完整的 PTH 比值可用于预测再次甲状旁腺切除术的致病甲状旁腺的定位。