Department of Neurology, Drexel University College of Medicine, Allegheny General Hospital, 4742 Centre Avenue, Apt 703, Pittsburgh, PA 15213, USA.
BMC Neurol. 2014 Mar 15;14:51. doi: 10.1186/1471-2377-14-51.
To review our experience using methotrexate as a single long-term immunosuppressant (IS) therapy in neuromyelitis optica/neuromyelitis optica spectrum disorders (NMO/NMOSD).
We performed a retrospective chart review of all patients with a diagnosis of NMO/NMOSD, supported by a positive NMO-IgG testing, who were treated with methotrexate. A paired sample 2 tailed t test was used to assess the annualized relapse rate during 18 months pre treatment with methotrexate to annualized relapse rate 18 months post treatment with methotrexate.
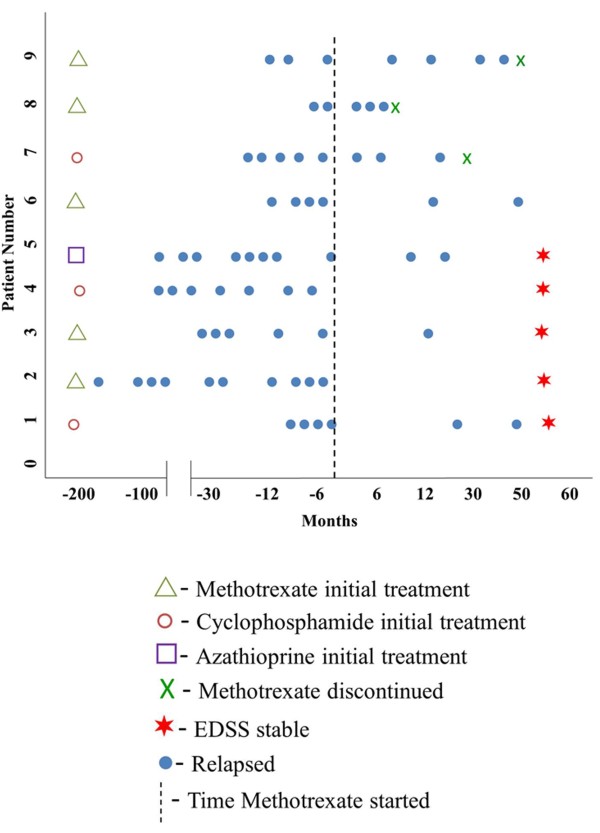
We followed 9 patients meeting criteria for the study for a median of 62 months. All patients were stabilized during attacks with high-dose steroids and/or plasmapheresis. Five patients (55.55%) were started on methotrexate as an initial long-term immunosuppressant strategy. Three patients (33.33%) were initially treated with pulse cyclophosphamide followed by methotrexate as a preplanned step-down strategy. One patient was started on azathioprine prior to methotrexate. No patient had side effects requiring change in methotrexate therapy. Five patients (55.55%) had stabilization of Expanded Disability Status Scale (EDSS) on methotrexate. One patient had a small increase in EDSS due to concomitant illness. Three patients (33.33%) had methotrexate treatment failure evidenced by worsening EDSS and ongoing relapses while on methotrexate, mandating a change in methotrexate therapy. Average annualized relapse rate in the entire group comparing 18 months prior versus 18 months after methotrexate treatment was reduced by an absolute value of 64% (3.11 vs 1.11). A paired t-test showed this reduction was highly significant (p = .009).
In our experience, methotrexate is safe and possibly efficacious as a single long-term IS therapy along with low dose corticosteroids that can reasonably be offered to patients with NMO/NMOSD.
回顾我们使用甲氨蝶呤作为视神经脊髓炎/视神经脊髓炎谱系疾病(NMO/NMOSD)单一长期免疫抑制剂(IS)治疗的经验。
我们对所有经 NMO-IgG 检测支持诊断为 NMO/NMOSD 的患者进行了回顾性图表审查,这些患者接受了甲氨蝶呤治疗。采用配对样本双侧 t 检验评估甲氨蝶呤治疗前 18 个月的年化复发率与甲氨蝶呤治疗后 18 个月的年化复发率。
我们对符合研究标准的 9 名患者进行了中位数为 62 个月的随访。所有患者在大剂量类固醇和/或血浆置换治疗下,病情在发作期间得到稳定。5 名患者(55.55%)开始使用甲氨蝶呤作为初始长期免疫抑制剂策略。3 名患者(33.33%)最初接受脉冲环磷酰胺治疗,然后作为预先计划的降级策略使用甲氨蝶呤。1 名患者在使用甲氨蝶呤之前开始使用硫唑嘌呤。没有患者因药物副作用需要改变甲氨蝶呤治疗方案。5 名患者(55.55%)在使用甲氨蝶呤时稳定了扩展残疾状态量表(EDSS)。1 名患者因并发疾病导致 EDSS略有增加。3 名患者(33.33%)在使用甲氨蝶呤时出现治疗失败,表现为 EDSS恶化和持续复发,需要改变甲氨蝶呤治疗方案。整个组别的平均年化复发率在甲氨蝶呤治疗前 18 个月与治疗后 18 个月相比降低了绝对值 64%(3.11 与 1.11)。配对 t 检验显示这种降低具有高度显著性(p=0.009)。
根据我们的经验,甲氨蝶呤联合低剂量皮质类固醇作为单一长期 IS 治疗是安全且可能有效的,可合理地提供给 NMO/NMOSD 患者。