Addison Christina L, Bouganim Nathaniel, Hilton John, Vandermeer Lisa, Dent Susan, Amir Eitan, Hopkins Sean, Kuchuk Iryna, Segal Roanne, Song Xinni, Gertler Stan, Mazzarello Sasha, Dranitsaris George, Ooi Daylily, Pond Gregory, Clemons Mark
Division of Medical Oncology, Ottawa Hospital Cancer Centre, 501 Smyth Road, Box 912, Ottawa, ON, K1H 8L6, Canada.
Breast Cancer Res Treat. 2014 Apr;144(3):615-24. doi: 10.1007/s10549-014-2906-x. Epub 2014 Mar 18.
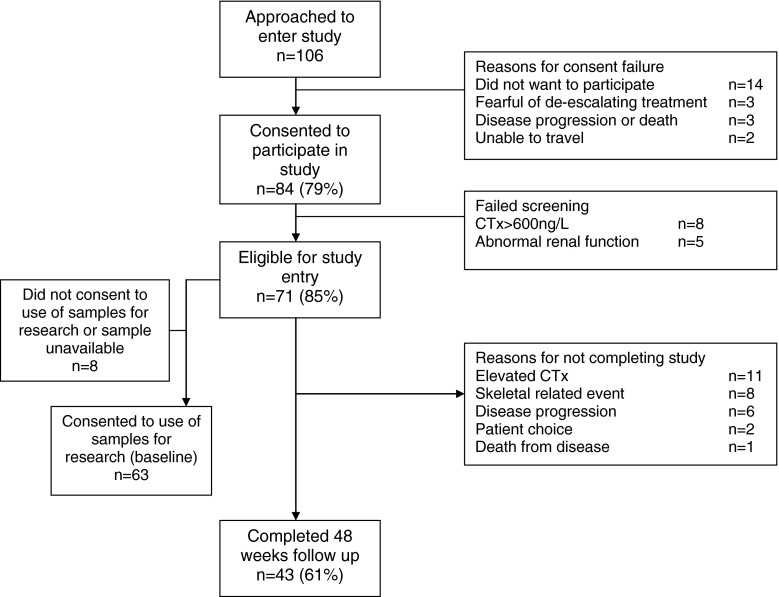
The optimal frequency of intravenous (IV) bisphosphonate administration is unclear. We thus performed a study evaluating the effects of switching from 3-4 to 12 weekly therapy in patients with biochemically defined low-risk bone metastases. Patients with serum C-telopeptide (CTx) levels ≤600 ng/L after ≥3 months of 3-4 weekly IV pamidronate were switched to 12 weekly therapy for 48 weeks. Primary endpoint was the proportion of patients maintaining CTx levels in the lower-risk range. All endpoints (serum CTx and bone-specific alkaline phosphatase (BSAP), skeletal-related events (SREs) and self-reported pain) were measured at baseline, 6, 12, 24, 36 and 48 weeks. Treatment failure was defined as biochemical failure (CTx > 600 ng/L) or a SRE. Exploratory biomarkers including; serum TGF-β, activin-A, bone sialoprotein (BSP), procollagen type 1 N-terminal propeptide and urinary N-telopeptide (NTx) were assessed at baseline as predictors for failure to complete treatment. Seventy-one patients accrued and 43 (61 %) completed 48 weeks of de-escalated therapy. Reasons for failure to complete treatment included; biochemical failure (CTx > 600 ng/L) (n = 10, 14.1 %), on-study SRE (n = 9, 12.7 %), disease progression (n = 7, 9.9 % including death from disease [n = 1, 1.4 %]) or patient choice (n = 2, 2.8 %). Elevated baseline levels of CTx, BSAP, NTx and BSP were associated with treatment failure. The majority of patients in this biochemically defined low-risk population could switch from 3-4 weekly to 12 weekly bisphosphonate therapy with no effect on CTx levels or SREs during the 48 week study. Larger trials are required to assess the roles of biomarkers as predictors of adequacy of de-escalated therapy.
静脉注射双膦酸盐的最佳给药频率尚不清楚。因此,我们开展了一项研究,评估生化指标定义的低风险骨转移患者从每3 - 4周一次治疗改为每12周一次治疗的效果。接受每3 - 4周静脉注射帕米膦酸≥3个月后血清I型胶原C端肽(CTx)水平≤600 ng/L的患者改为每12周治疗一次,持续48周。主要终点是CTx水平维持在低风险范围的患者比例。在基线、第6、12、24、36和48周测量所有终点指标(血清CTx和骨特异性碱性磷酸酶(BSAP)、骨相关事件(SREs)和自我报告的疼痛)。治疗失败定义为生化失败(CTx > 600 ng/L)或发生骨相关事件。在基线时评估包括血清转化生长因子-β、激活素-A、骨唾液蛋白(BSP)、I型前胶原N端前肽和尿I型胶原C端肽(NTx)在内的探索性生物标志物,作为未能完成治疗的预测指标。共纳入71例患者,43例(61%)完成了48周的降阶梯治疗。未完成治疗的原因包括:生化失败(CTx > 600 ng/L)(10例,14.1%)、研究期间发生骨相关事件(9例,12.7%)、疾病进展(7例,9.9%,包括因疾病死亡[1例,1.4%])或患者选择(2例,2.8%)。CTx、BSAP、NTx和BSP的基线水平升高与治疗失败相关。在这项生化指标定义的低风险人群中,大多数患者可以从每3 - 4周一次改为每12周一次双膦酸盐治疗,在48周的研究期间对CTx水平或骨相关事件无影响。需要更大规模的试验来评估生物标志物作为降阶梯治疗充分性预测指标的作用。