Institute of Neuropathology, University Hospital Zurich, Zurich, Switzerland; Department of Neurology, University Hospital Basel, Basel, Switzerland.
Department of Neurology, University Hospital Basel, Basel, Switzerland; Department of Neurology, University Hospital Zurich, Zurich, Switzerland.
PLoS One. 2014 Mar 19;9(3):e92421. doi: 10.1371/journal.pone.0092421. eCollection 2014.
In this study, we assessed the relationship of insular strokes and plasma MR-proANP levels with newly diagnosed atrial fibrillation (NDAF).
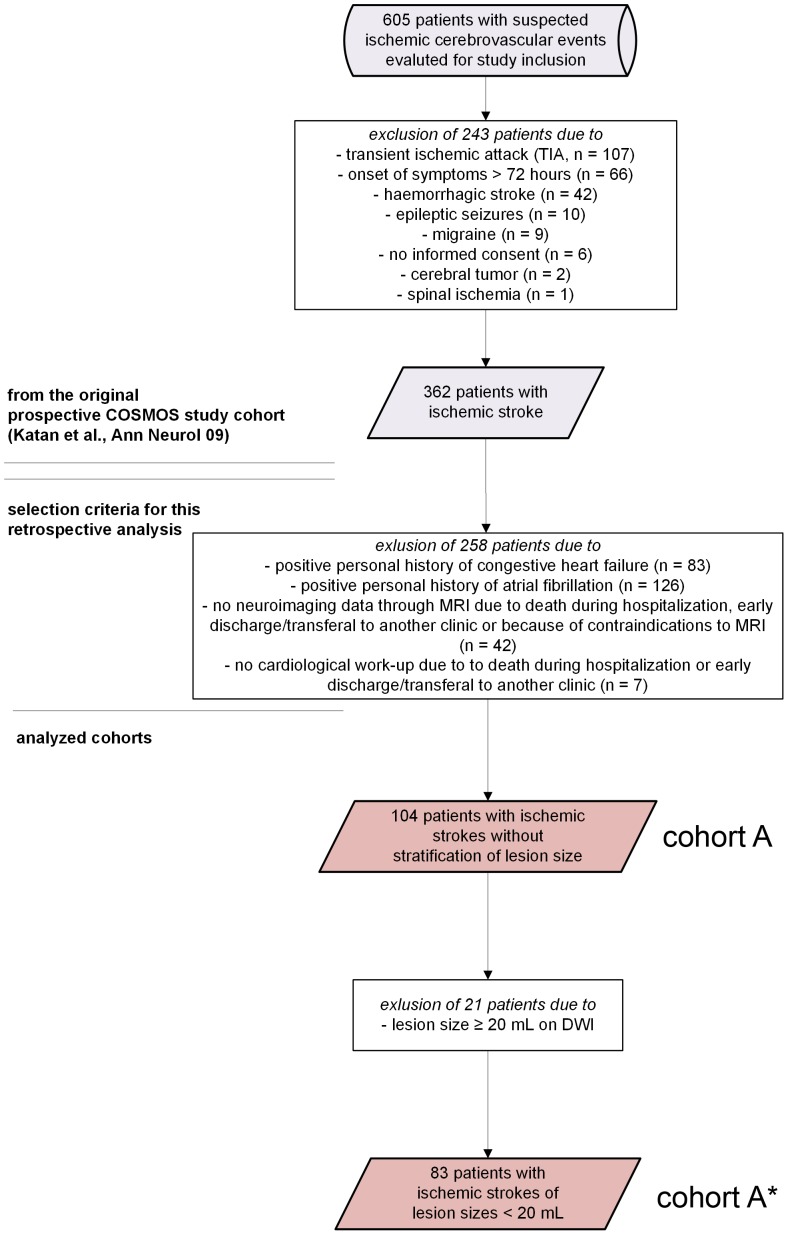
This study is based on a prospective acute stroke cohort (http://www.clinicaltrials.gov, NCT00390962). Patient eligibility was dependent on the diagnosis of acute ischemic stroke, absence of previous stroke based on past medical history and MRI, no history of AF and congestive heart failure (cohort A) and, additionally, no stroke lesion size ≥ 20 mL (sub-cohort A*). AF, the primary endpoint, was detected on 24-hour electrocardiography and/or echocardiography. Involvement of the insula was assessed by two experienced readers on MRI blinded to clinical data. MR-proANP levels were obtained through a novel sandwich immunoassay. Logistic-regression-models were fitted to estimate odds ratios for the association of insular strokes and MR-proANP with NDAF. The discriminatory accuracy of insular strokes and MR-proANP was assessed by a model-wise comparison of the area under the receiver-operating-characteristics-curve (AUC) with known predictors of AF.
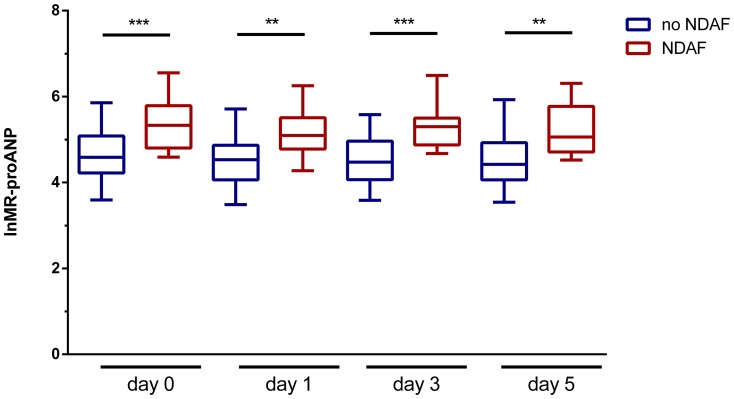
104 (cohort A) and 83 (cohort A*) patients fulfilled above-mentioned criteria. Patients with isolated insular strokes had a 10.7-fold higher odds of NDAF than patients with a small ischemic stroke at any other location. The AUC of multivariate logistic regression models for the prediction of NDAF improved significantly when adding stroke location and MR-proANP levels. Moreover, MR-proANP levels remained significantly elevated throughout the acute hospitalization period in patients with NDAF compared to those without.
Isolated insular strokes and plasma MR-proANP levels on admission are independent predictors of NDAF and significantly improve the prediction accuracy of identifying patients with NDAF compared to known predictors including age, the NIHSS and lesion size. To accelerate accurate diagnosis and enhance secondary prevention in acute stroke, higher levels of MR-proANP and insular strokes may represent easily accessible indicators of AF if confirmed in an independent validation cohort.
本研究旨在评估脑岛梗死与血浆 MR-proANP 水平与新发心房颤动(NDAF)之间的关系。
本研究基于前瞻性急性卒中队列(http://www.clinicaltrials.gov,NCT00390962)。患者入选标准取决于急性缺血性卒中的诊断、既往病史和 MRI 无先前卒中、无 AF 和充血性心力衰竭(队列 A),此外,还需要无梗死灶大小≥20mL(亚组 A*)。AF 作为主要终点,通过 24 小时心电图和/或超声心动图进行检测。两名经验丰富的 MRI 阅读者对脑岛的受累情况进行评估,评估时对临床数据不知情。通过新型夹心免疫分析法获得 MR-proANP 水平。使用逻辑回归模型来估计脑岛梗死和 MR-proANP 与 NDAF 的关联的优势比。通过比较不同模型的接收者操作特征曲线下面积(AUC)来评估脑岛梗死和 MR-proANP 的诊断准确性,与已知的 AF 预测因子进行比较。
104 名(队列 A)和 83 名(队列 A*)患者符合上述标准。孤立性脑岛梗死患者发生 NDAF 的几率是其他任何部位小面积缺血性卒中患者的 10.7 倍。当加入卒中部位和 MR-proANP 水平时,用于预测 NDAF 的多变量逻辑回归模型的 AUC 显著改善。此外,与无 NDAF 的患者相比,有 NDAF 的患者的 MR-proANP 水平在整个急性住院期间持续升高。
孤立性脑岛梗死和入院时的血浆 MR-proANP 水平是 NDAF 的独立预测因子,与包括年龄、NIHSS 和病变大小在内的已知预测因子相比,显著提高了识别 NDAF 患者的预测准确性。如果在独立验证队列中得到证实,较高的 MR-proANP 水平和脑岛梗死可能代表易于获得的 AF 指标,以加速急性卒中的准确诊断和加强二级预防。