Burger Emily A, Sy Stephen, Nygård Mari, Kristiansen Ivar S, Kim Jane J
University of Oslo, Department of Health Management and Health Economics, Oslo, Norway.
Harvard School of Public Health, Department of Health Policy and Management, Center for Health Decision Science Boston, Massachusetts, United States of America.
PLoS One. 2014 Mar 20;9(3):e89974. doi: 10.1371/journal.pone.0089974. eCollection 2014.
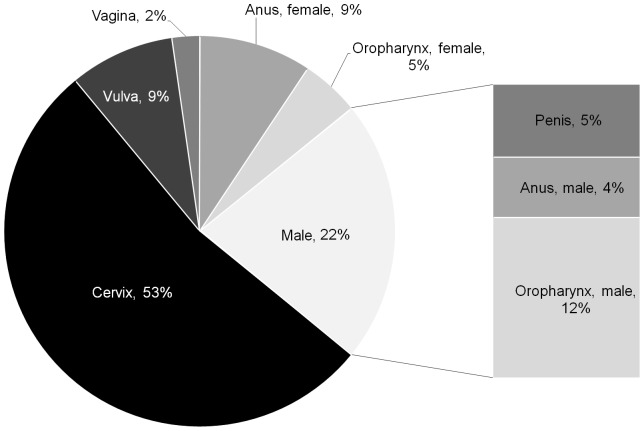
Increasingly, countries have introduced female vaccination against human papillomavirus (HPV), causally linked to several cancers and genital warts, but few have recommended vaccination of boys. Declining vaccine prices and strong evidence of vaccine impact on reducing HPV-related conditions in both women and men prompt countries to reevaluate whether HPV vaccination of boys is warranted.
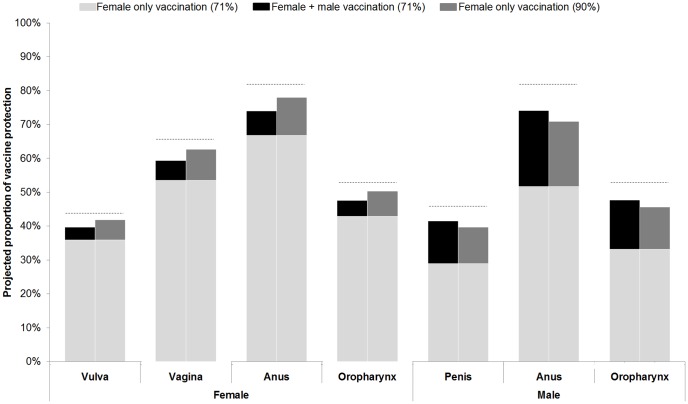
A previously-published dynamic model of HPV transmission was empirically calibrated to Norway. Reductions in the incidence of HPV, including both direct and indirect benefits, were applied to a natural history model of cervical cancer, and to incidence-based models for other non-cervical HPV-related diseases. We calculated the health outcomes and costs of the different HPV-related conditions under a gender-neutral vaccination program compared to a female-only program.
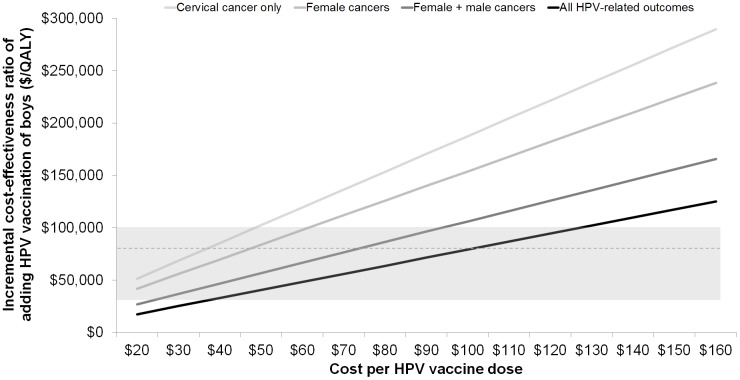
Vaccine price had a decisive impact on results. For example, assuming 71% coverage, high vaccine efficacy and a reasonable vaccine tender price of $75 per dose, we found vaccinating both girls and boys fell below a commonly cited cost-effectiveness threshold in Norway ($83,000/quality-adjusted life year (QALY) gained) when including vaccine benefit for all HPV-related diseases. However, at the current market price, including boys would not be considered 'good value for money.' For settings with a lower cost-effectiveness threshold ($30,000/QALY), it would not be considered cost-effective to expand the current program to include boys, unless the vaccine price was less than $36/dose. Increasing vaccination coverage to 90% among girls was more effective and less costly than the benefits achieved by vaccinating both genders with 71% coverage.
At the anticipated tender price, expanding the HPV vaccination program to boys may be cost-effective and may warrant a change in the current female-only vaccination policy in Norway. However, increasing coverage in girls is uniformly more effective and cost-effective than expanding vaccination coverage to boys and should be considered a priority.
越来越多的国家已推行针对人乳头瘤病毒(HPV)的女性疫苗接种,HPV与多种癌症及生殖器疣存在因果关联,但很少有国家建议对男孩进行疫苗接种。疫苗价格下降以及有强有力的证据表明疫苗对降低女性和男性HPV相关病症有效果,促使各国重新评估对男孩进行HPV疫苗接种是否必要。
先前发布的HPV传播动态模型依据挪威实际情况进行校准。将HPV发病率的降低(包括直接和间接益处)应用于宫颈癌自然史模型以及其他非宫颈癌HPV相关疾病的基于发病率的模型。我们计算了与仅针对女性的疫苗接种计划相比,在性别中立的疫苗接种计划下不同HPV相关病症的健康结果和成本。
疫苗价格对结果有决定性影响。例如,假设覆盖率为71%、疫苗效力高且每剂疫苗招标价格合理为75美元,我们发现当将所有HPV相关疾病的疫苗益处纳入考量时,在挪威对女孩和男孩都进行接种低于普遍引用的成本效益阈值(每获得一个质量调整生命年(QALY)83,000美元)。然而,按照当前市场价格,将男孩纳入接种不被认为“物有所值”。对于成本效益阈值较低(每QALY 30,000美元)的情况,将当前计划扩大到包括男孩不被认为具有成本效益,除非疫苗价格低于每剂36美元。将女孩的疫苗接种覆盖率提高到90%比男女接种覆盖率均为71%所获得的益处更有效且成本更低。
按照预期的招标价格,将HPV疫苗接种计划扩大到男孩可能具有成本效益,可能有必要改变挪威当前仅针对女性的疫苗接种政策。然而,提高女孩的接种覆盖率始终比扩大男孩的接种覆盖率更有效且更具成本效益,应被视为优先事项。