Pearson Amber L, Kvizhinadze Giorgi, Wilson Nick, Smith Megan, Canfell Karen, Blakely Tony
Department of Public Health, University of Otago, 23A Mein Street, Wellington 6242, New Zealand.
BMC Infect Dis. 2014 Jun 26;14:351. doi: 10.1186/1471-2334-14-351.
Similar to many developed countries, vaccination against human papillomavirus (HPV) is provided only to girls in New Zealand and coverage is relatively low (47% in school-aged girls for dose 3). Some jurisdictions have already extended HPV vaccination to school-aged boys. Thus, exploration of the cost-utility of adding boys' vaccination is relevant. We modeled the incremental health gain and costs for extending the current girls-only program to boys, intensifying the current girls-only program to achieve 73% coverage, and extension of the intensive program to boys.
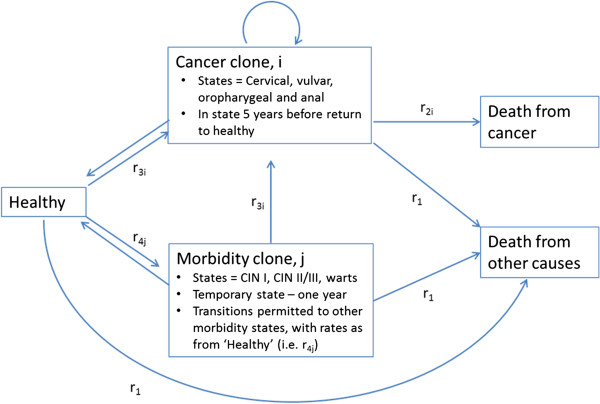
A Markov macro-simulation model, which accounted for herd immunity, was developed for an annual cohort of 12-year-olds in 2011 and included the future health states of: cervical cancer, pre-cancer (CIN I to III), genital warts, and three other HPV-related cancers. In each state, health sector costs, including additional health costs from extra life, and quality-adjusted life-years (QALYs) were accumulated. The model included New Zealand data on cancer incidence and survival, and other cause mortality (all by sex, age, ethnicity and deprivation).
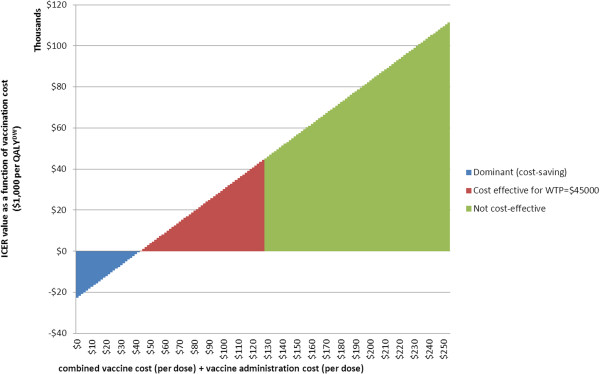
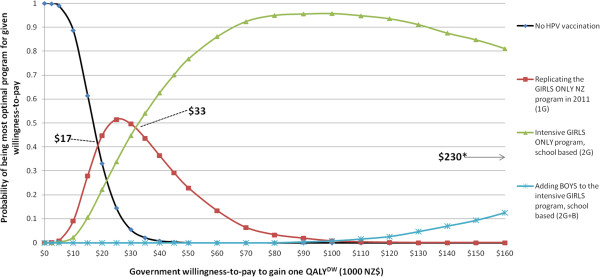
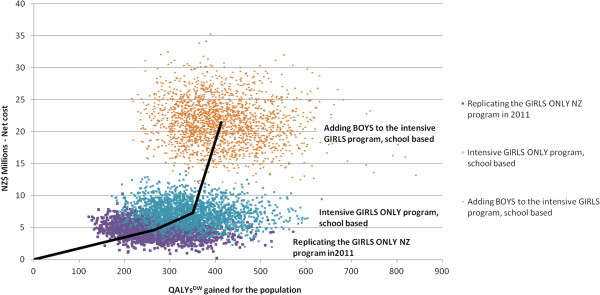
At an assumed local willingness-to-pay threshold of US$29,600, vaccination of 12-year-old boys to achieve the current coverage for girls would not be cost-effective, at US$61,400/QALY gained (95% UI $29,700 to $112,000; OECD purchasing power parities) compared to the current girls-only program, with an assumed vaccine cost of US$59 (NZ$113). This was dominated though by the intensified girls-only program; US$17,400/QALY gained (95% UI: dominant to $46,100). Adding boys to this intensified program was also not cost-effective; US$128,000/QALY gained, 95% UI: $61,900 to $247,000).Vaccination of boys was not found to be cost-effective, even for additional scenarios with very low vaccine or program administration costs - only when combined vaccine and administration costs were NZ$125 or lower per dose was vaccination of boys cost-effective.
These results suggest that adding boys to the girls-only HPV vaccination program in New Zealand is highly unlikely to be cost-effective. In order for vaccination of males to become cost-effective in New Zealand, vaccine would need to be supplied at very low prices and administration costs would need to be minimised.
与许多发达国家类似,新西兰仅为女孩提供人乳头瘤病毒(HPV)疫苗接种,接种率相对较低(学龄女孩第三剂接种率为47%)。一些司法管辖区已将HPV疫苗接种扩展至学龄男孩。因此,探讨增加男孩接种疫苗的成本效益具有现实意义。我们对将当前仅针对女孩的项目扩展至男孩、强化当前仅针对女孩的项目以实现73%的接种率以及将强化项目扩展至男孩的增量健康收益和成本进行了建模。
针对2011年一组12岁儿童建立了一个考虑群体免疫的马尔可夫宏观模拟模型,其中包括宫颈癌、癌前病变(CIN I至III级)、尖锐湿疣以及其他三种HPV相关癌症的未来健康状态。在每种状态下,累积卫生部门成本,包括因延长寿命产生的额外卫生成本以及质量调整生命年(QALY)。该模型纳入了新西兰癌症发病率和生存率以及其他死因死亡率的数据(均按性别、年龄、种族和贫困程度分类)。
假设当地支付意愿阈值为29,600美元,为12岁男孩接种疫苗以达到当前女孩的接种率不具有成本效益,每获得一个QALY需花费61,400美元(95%可信区间为29,700美元至112,000美元;经合组织购买力平价),而当前仅针对女孩的项目,假设疫苗成本为59美元(113新西兰元)。不过,强化后的仅针对女孩的项目占主导地位;每获得一个QALY花费17,400美元(95%可信区间:占主导地位至46,100美元)。将男孩纳入这一强化项目也不具有成本效益;每获得一个QALY花费128,000美元,95%可信区间为61,900美元至247,000美元。即使在疫苗或项目管理成本极低的其他情况下,男孩接种疫苗也不具有成本效益——只有当疫苗和管理成本每剂降至125新西兰元或更低时,男孩接种疫苗才具有成本效益。
这些结果表明,在新西兰仅针对女孩的HPV疫苗接种项目中增加男孩接种极不可能具有成本效益。为使新西兰男性接种疫苗具有成本效益,疫苗需以极低价格供应,且管理成本需降至最低。