Konstantinidis Ioannis T, Do Richard K G, Gultekin David H, Gönen Mithat, Schwartz Lawrence H, Fong Yuman, Allen Peter J, D'Angelica Michael I, DeMatteo Ronald P, Klimstra David S, Kemeny Nancy E, Jarnagin William R
Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, NY, USA,
Ann Surg Oncol. 2014 Aug;21(8):2675-83. doi: 10.1245/s10434-014-3649-y. Epub 2014 Mar 25.
For patients with unresectable intrahepatic cholangiocarcinoma (ICC), treatment options are limited and survival is poor. This study summarizes the long-term outcome of two previously reported clinical trials using hepatic arterial infusion (HAI) with floxuridine and dexamethasone (with or without bevacizumab) in advanced ICC.
Prospectively collected clinicopathologic and survival data were retrospectively reviewed. Response was based on Response Evaluation Criteria in Solid Tumors (RECIST). Pre-HAI dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) images were reviewed, and tumor perfusion data correlated with outcome.
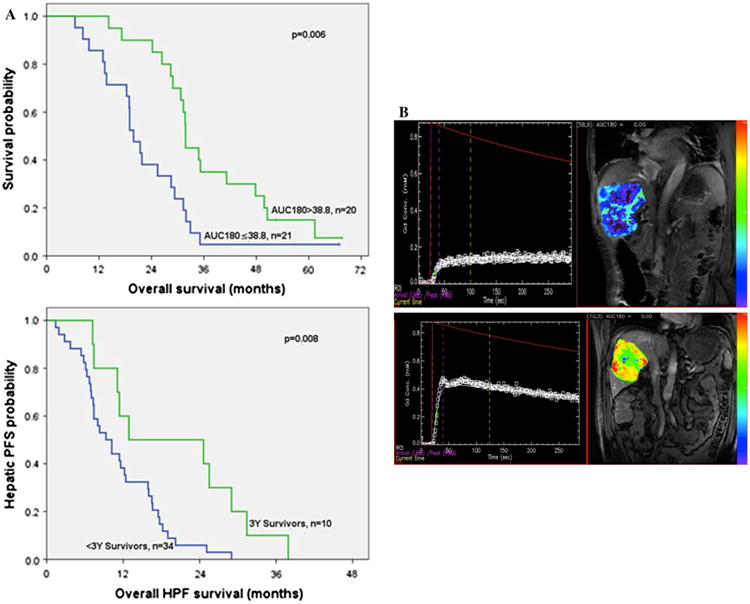
Forty-four patients were analyzed (floxuridine, 26; floxuridine/bevacizumab, 18). At a median follow-up of 29.3 months, 41 patients had died of disease. Partial response by RECIST was observed in 48 %, and 50 % had stable disease. Three patients underwent resection after response, and 82 % received additional HAI after removal from the trials. Median survival was similar in both trials (floxuridine 29.3 months vs. floxuridine/bevacizumab 28.5 months; p = 0.96). Ten (23 %) patients survived ≥3 years, including 5 (11 %) who survived ≥5 years. Tumor perfusion measured on pre-treatment DCE-MRI [area under the gadolinium concentration curve at 90 and 180 s (AUC90 and AUC180, respectively)] was significantly higher in ≥3-year survivors and was the only factor that distinguished this group from <3-year survivors (mean AUC90 22.6 vs. 15.9 mM s, p = 0.025, and mean AUC180 48.9 vs. 32.3 mM s, p = 0.003, respectively). Median hepatic progression-free survival was longer in ≥3-year survivors (12.9 vs. 9.3 months, respectively; p = 0.008).
HAI chemotherapy can result in prolonged survival in unresectable ICC. Pre-HAI DCE-MRI may predict treatment outcome.
对于无法切除的肝内胆管癌(ICC)患者,治疗选择有限且生存率较低。本研究总结了两项先前报道的关于在晚期ICC中使用氟尿苷和地塞米松(联合或不联合贝伐单抗)进行肝动脉灌注(HAI)治疗的临床试验的长期结果。
对前瞻性收集的临床病理和生存数据进行回顾性分析。疗效根据实体瘤疗效评价标准(RECIST)进行评估。回顾HAI前的动态对比增强磁共振成像(DCE-MRI)图像,并将肿瘤灌注数据与预后相关联。
分析了44例患者(氟尿苷组26例;氟尿苷/贝伐单抗组18例)。中位随访29.3个月时,41例患者死于疾病。根据RECIST标准观察到部分缓解率为48%,疾病稳定率为50%。3例患者在缓解后接受了手术切除,82%的患者在退出试验后接受了额外的HAI治疗。两项试验的中位生存期相似(氟尿苷组29.3个月 vs. 氟尿苷/贝伐单抗组28.5个月;p = 0.96)。10例(23%)患者存活≥3年,其中5例(11%)存活≥5年。在≥3年生存者中,治疗前DCE-MRI测量的肿瘤灌注[钆浓度曲线在90秒和180秒时的面积(分别为AUC90和AUC180)]显著更高,且是将该组与<3年生存者区分开来的唯一因素(平均AUC90分别为22.6 vs. 15.9 mM·s,p = 0.025;平均AUC180分别为48.9 vs. 32.3 mM·s,p = 0.003)。≥3年生存者的中位肝无进展生存期更长(分别为12.9 vs. 9.3个月;p = 0.008)。
HAI化疗可延长无法切除的ICC患者的生存期。HAI前的DCE-MRI可能预测治疗结果。