Wu Huang-Hui, Wang Hong-Tao, Jin Jun-Jie, Cui Guang-Bin, Zhou Ke-Cheng, Chen Yu, Chen Guo-Zhong, Dong Yu-Lin, Wang Wen
Department of Anesthesiology, Fuzhou General Hospital of Nanjing Military Region, Fuzhou, PR China; Unit for Evidence Based Medicine, Department of Anatomy, Histology and Embryology & K.K. Leung Brain Research Centre, Preclinical School of Medicine, Fourth Military Medical University, Xi'an, PR China.
Unit for Evidence Based Medicine, Department of Anatomy, Histology and Embryology & K.K. Leung Brain Research Centre, Preclinical School of Medicine, Fourth Military Medical University, Xi'an, PR China; Department of Burn and Cutaneous Surgery, Xi'jing Hospital, Fourth Military Medical University, Xi'an, PR China.
PLoS One. 2014 Mar 26;9(3):e93114. doi: 10.1371/journal.pone.0093114. eCollection 2014.
Neuraxial application of dexmedetomidine (DEX) as adjuvant analgesic has been invetigated in some randomized controlled trials (RCTs) but not been approved because of the inconsistency of efficacy and safety in these RCTs. We performed this meta-analysis to access the efficacy and safety of neuraxial DEX as local anaesthetic (LA) adjuvant.
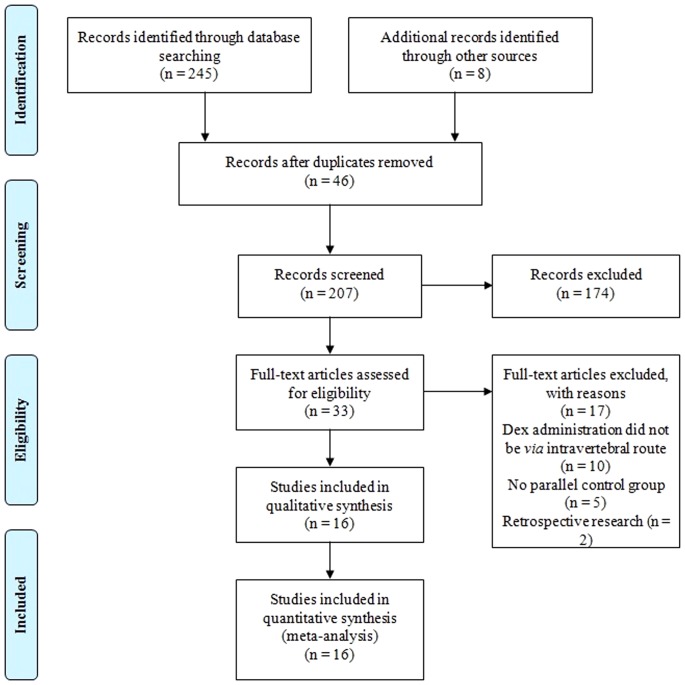
We searched PubMed, PsycINFO, Scopus, EMBASE, and CENTRAL databases from inception to June 2013 for RCTs that investigated the analgesia efficacy and safety for neuraxial application DEX as LA adjuvant. Effects were summarized using standardized mean differences (SMDs), weighed mean differences (WMDs) or odds ratio (OR) with suitable effect model. The primary outcomes were postoperative pain intensity and analgesic duration, bradycardia and hypotension.
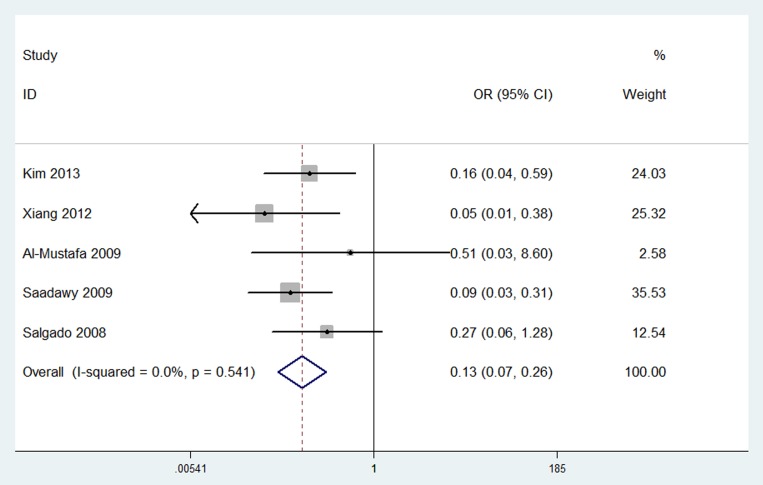
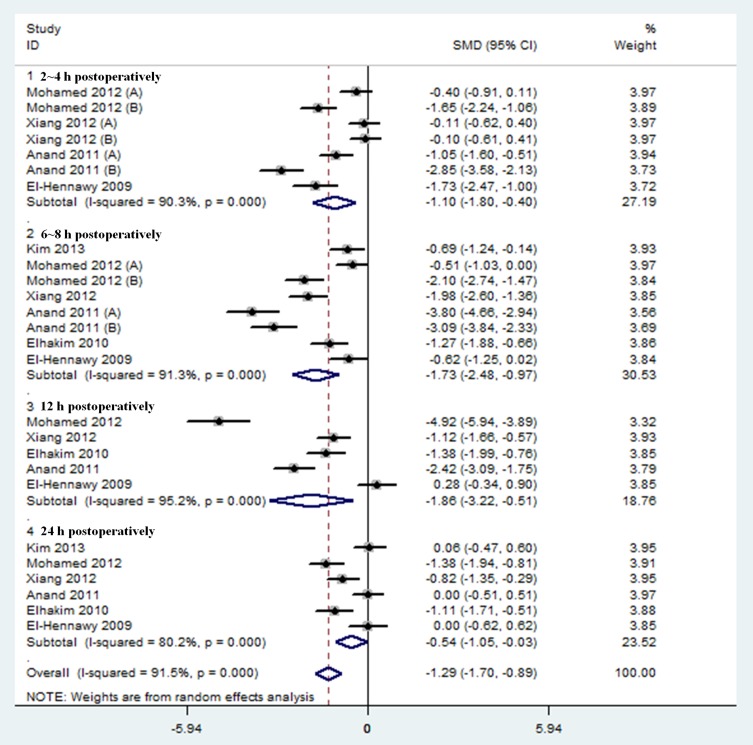
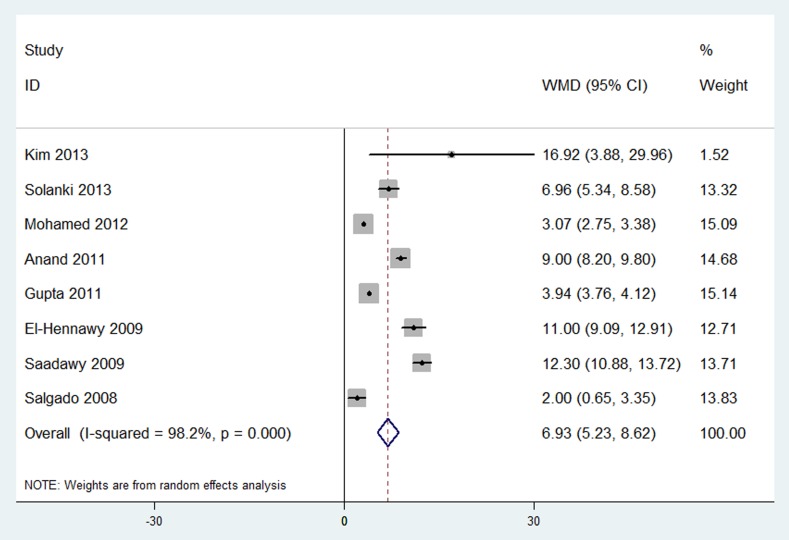
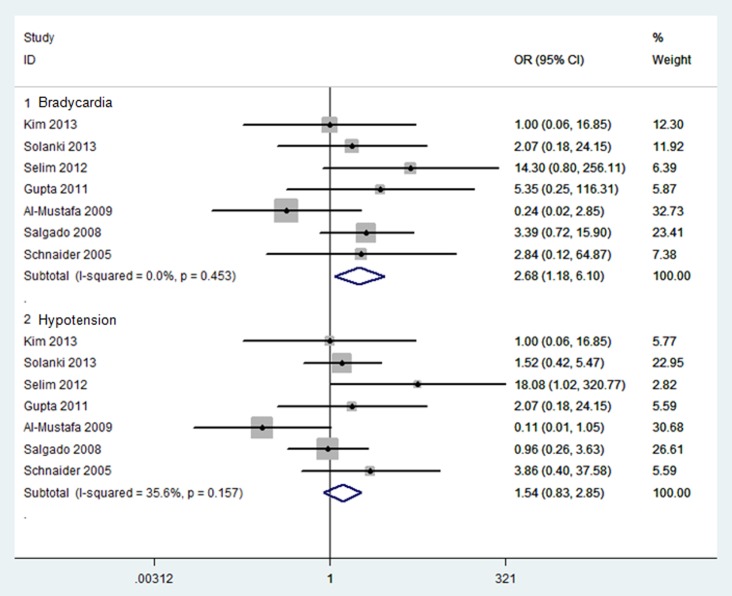
Sixteen RCTs involving 1092 participants were included. Neuraxial DEX significantly decreased postoperative pain intensity (SMD, -1.29; 95% confidence interval (CI), -1.70 to -0.89; P<0.00001), prolonged analgesic duration (WMD, 6.93 hours; 95% CI, 5.23 to 8.62; P<0.00001) and increased the risk of bradycardia (OR, 2.68; 95% CI, 1.18 to 6.10; P = 0.02). No evidence showed that neuraxial DEX increased the risk of other adverse events, such as hypotension (OR, 1.54; 95% CI, 0.83 to 2.85; P = 0.17). Additionally, neuraxial DEX was associated with beneficial alterations in postoperative sedation scores and number of analgesic requirements, sensory and motor block characteristics, and intro-operative hemodynamics.
Neuraxial DEX is a favorable LA adjuvant with better and longer analgesia. The greatest concern is bradycardia. Further large sample trials with strict design and focusing on long-term outcomes are needed.
右美托咪定(DEX)用于椎管内作为辅助镇痛药已在一些随机对照试验(RCT)中进行了研究,但由于这些RCT中疗效和安全性的不一致性,尚未获得批准。我们进行这项荟萃分析以评估椎管内应用DEX作为局部麻醉药(LA)辅助剂的疗效和安全性。
我们检索了从数据库建立至2013年6月的PubMed、PsycINFO、Scopus、EMBASE和CENTRAL数据库,以查找研究椎管内应用DEX作为LA辅助剂的镇痛疗效和安全性的RCT。使用标准化均数差(SMD)、加权均数差(WMD)或比值比(OR)以及合适的效应模型汇总效应。主要结局为术后疼痛强度、镇痛持续时间、心动过缓和低血压。
纳入了16项涉及1092名参与者的RCT。椎管内应用DEX可显著降低术后疼痛强度(SMD,-1.29;95%置信区间(CI),-1.70至-0.89;P<0.00001),延长镇痛持续时间(WMD,6.93小时;95%CI,5.23至8.62;P<0.00001),并增加心动过缓的风险(OR,2.68;95%CI,1.18至6.10;P = 0.02)。没有证据表明椎管内应用DEX会增加其他不良事件的风险,如低血压(OR,1.54;95%CI,0.83至2.85;P = 0.17)。此外,椎管内应用DEX与术后镇静评分、镇痛需求次数、感觉和运动阻滞特征以及术中血流动力学的有益改变有关。
椎管内应用DEX是一种良好的LA辅助剂,具有更好、更持久的镇痛效果。最值得关注的是心动过缓。需要进一步进行设计严格且关注长期结局的大样本试验。