Puig Ignasi, Calvet Xavier, Baylina Mireia, Isava Álvaro, Sort Pau, Llaó Jordina, Porta Francesc, Vida Francesc
Digestive Diseases Department, Althaia Xarxa Assistencial Universitària de Manresa, Barcelona, Spain; Universitat Internacional de Catalunya, Barcelona, Spain; Departament de Medicina, Universitat Autònoma de Barcelona, Barcelona, Spain.
Departament de Medicina, Universitat Autònoma de Barcelona, Barcelona, Spain; Digestive Diseases Department, Corporació Sanitària Parc Taulí, Sabadell, Barcelona, Spain; Centro de Investigación Biomédica en Red de enfermedades hepáticas y digestivas (CIBERehd), Madrid, Spain.
PLoS One. 2014 Mar 27;9(3):e92922. doi: 10.1371/journal.pone.0092922. eCollection 2014.
Non-steroidal anti-inflammatory drugs (NSAIDs) have been shown to be efficacious to prevent pancreatitis after endoscopic retrograde cholangiopancreatography (ERCP). However, the target patients, the type of NSAID, the route of administration and the time of drug delivery remain unclear, as well as the potential efficacy in reducing the severity of pancreatitis, length of hospital stay and mortality. The objective of the study was to evaluate these questions by performing a systematic review and meta-analysis.
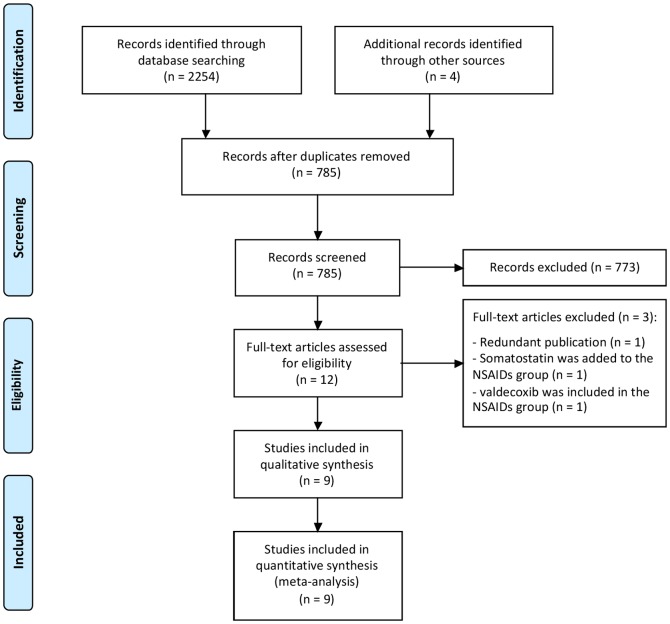
Multiple searches were performed in the main databases. Randomized controlled trials (RCTs) comparing NSAIDs vs. placebo in the prevention of post-ERCP pancreatitis were included. Primary endpoint of the study was the efficacy for pancreatitis prevention. Sub-analyses were performed to determine the risk reduction in high and low risk patients, and to define optimal time, route of administration, and type of NSAID. Secondary endpoints were safety, moderate to severe pancreatitis prevention and reduction of hospital stay and mortality.
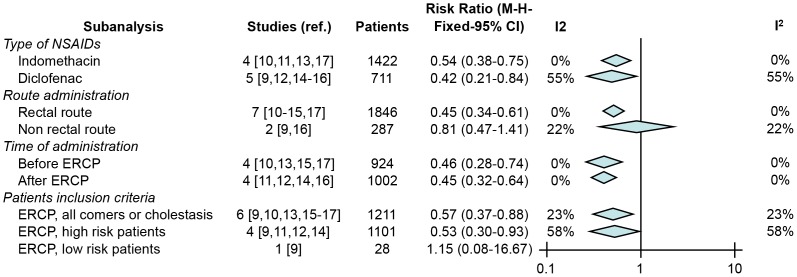
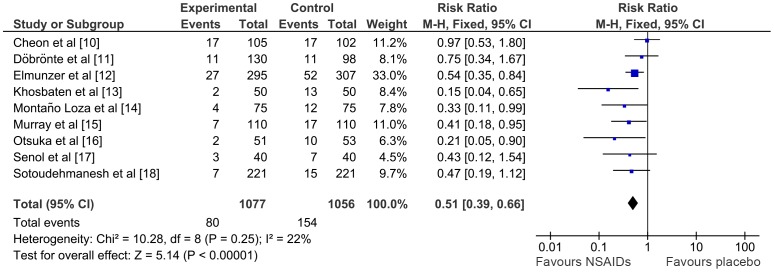
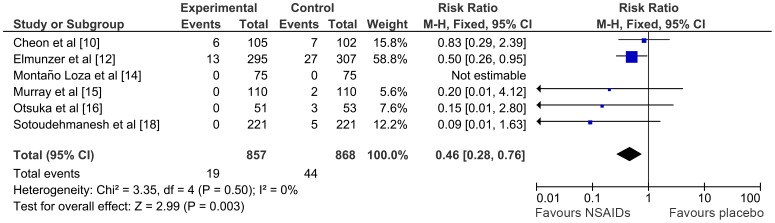
Nine RCTs enrolling 2133 patients were included. The risk of pancreatitis was lower in the NSAID group than in the placebo group (RR 0.51; 95%CI 0.39-0.66). The number needed to treat was 14. The risk of moderate to severe pancreatitis was also lower in the NSAID group. (RR 0.46; 95%CI 0.28-0.76). No adverse events related to NSAID use were reported. NSAIDs were effective in both high-risk and unselected patients (RR 0.53; 95%CI 0.30-0.93 and RR 0.57; 95%CI 0.37-0.88). In the subanalyses, only rectal administration of either indomethacin (RR 0.54; 95%CI 0.38-0.75) or diclofenac (RR 0.42; 95%CI 0.21-0.84) was shown to be effective. There were not enough data to perform a meta-analysis in hospital stay reduction. No deaths occurred.
A single rectal dose of indomethacin or diclofenac before or immediately after ERCP is safe and prevents procedure-related pancreatitis both in high risk and in unselected patients.
非甾体抗炎药(NSAIDs)已被证明在预防内镜逆行胰胆管造影(ERCP)术后胰腺炎方面有效。然而,目标患者、NSAID的类型、给药途径和给药时间仍不明确,以及在降低胰腺炎严重程度、住院时间和死亡率方面的潜在疗效也不明确。本研究的目的是通过进行系统评价和荟萃分析来评估这些问题。
在主要数据库中进行了多次检索。纳入了比较NSAIDs与安慰剂预防ERCP术后胰腺炎的随机对照试验(RCTs)。该研究的主要终点是预防胰腺炎的疗效。进行亚组分析以确定高风险和低风险患者的风险降低情况,并确定最佳时间、给药途径和NSAID的类型。次要终点是安全性、预防中度至重度胰腺炎以及缩短住院时间和降低死亡率。
纳入了9项RCTs,共2133例患者。NSAID组胰腺炎的风险低于安慰剂组(RR 0.51;95%CI 0.39 - 0.66)。治疗所需人数为14。NSAID组中度至重度胰腺炎的风险也较低(RR 0.46;95%CI 0.28 - 0.76)。未报告与使用NSAIDs相关的不良事件。NSAIDs在高风险患者和未选择的患者中均有效(RR 0.53;95%CI 0.30 - 0.93和RR 0.57;95%CI 0.37 - 0.88)。在亚组分析中,仅吲哚美辛(RR 0.54;95%CI 0.38 - 0.75)或双氯芬酸(RR 0.42;95%CI 0.21 - 0.84)的直肠给药显示有效。没有足够的数据进行缩短住院时间的荟萃分析。未发生死亡。
在ERCP前或后立即给予单次直肠剂量的吲哚美辛或双氯芬酸是安全的,并且在高风险患者和未选择的患者中均可预防与手术相关的胰腺炎。