Kirk A D, Guasch A, Xu H, Cheeseman J, Mead S I, Ghali A, Mehta A K, Wu D, Gebel H, Bray R, Horan J, Kean L S, Larsen C P, Pearson T C
Emory Transplant Center, Emory University, Atlanta, GA.
Am J Transplant. 2014 May;14(5):1142-51. doi: 10.1111/ajt.12712. Epub 2014 Mar 31.
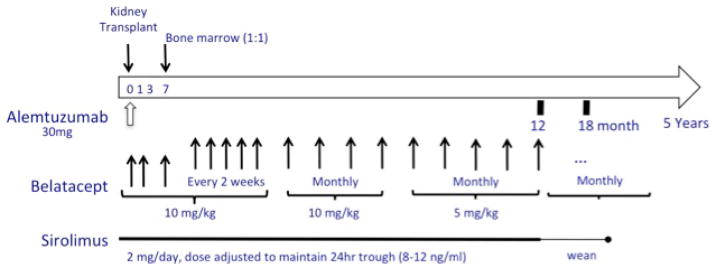
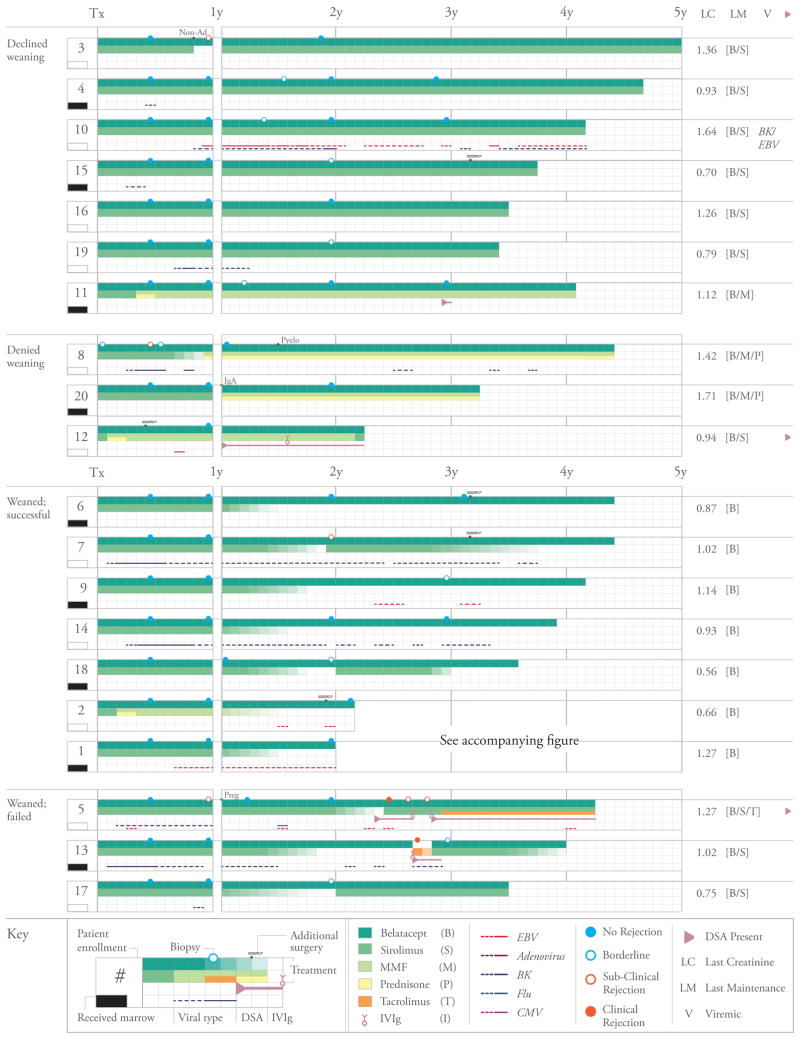
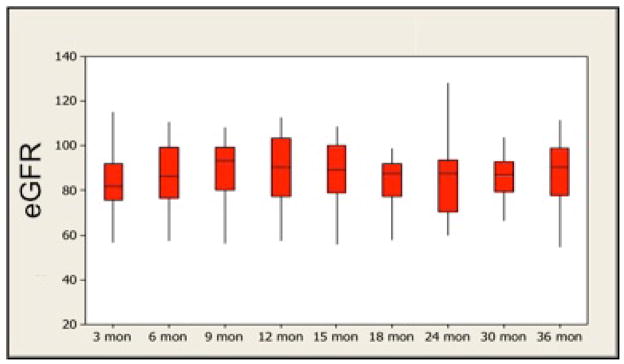
Kidney transplantation remains limited by toxicities of calcineurin inhibitors (CNIs) and steroids. Belatacept is a less toxic CNI alternative, but existing regimens rely on steroids and have higher rejection rates. Experimentally, donor bone marrow and sirolimus promote belatacept's efficacy. To investigate a belatacept-based regimen without CNIs or steroids, we transplanted recipients of live donor kidneys using alemtuzumab induction, monthly belatacept and daily sirolimus. Patients were randomized 1:1 to receive unfractionated donor bone marrow. After 1 year, patients were allowed to wean from sirolimus. Patients were followed clinically and with surveillance biopsies. Twenty patients were transplanted, all successfully. Mean creatinine (estimated GFR) was 1.10 ± 0.07 mg/dL (89 ± 3.56 mL/min) and 1.13 ± 0.07 mg/dL (and 88 ± 3.48 mL/min) at 12 and 36 months, respectively. Excellent results were achieved irrespective of bone marrow infusion. Ten patients elected oral immunosuppressant weaning, seven of whom were maintained rejection-free on monotherapy belatacept. Those failing to wean were successfully maintained on belatacept-based regimens supplemented by oral immunosuppression. Seven patients declined immunosuppressant weaning and three patients were denied weaning for associated medical conditions; all remained rejection-free. Belatacept and sirolimus effectively prevent kidney allograft rejection without CNIs or steroids when used following alemtuzumab induction. Selected, immunologically low-risk patients can be maintained solely on once monthly intravenous belatacept.
肾移植仍然受到钙调神经磷酸酶抑制剂(CNIs)和类固醇毒性的限制。贝拉西普是一种毒性较小的CNI替代药物,但现有的治疗方案依赖类固醇且排斥率较高。在实验中,供体骨髓和西罗莫司可提高贝拉西普的疗效。为了研究一种不使用CNIs或类固醇的基于贝拉西普的治疗方案,我们对活体供肾受者进行了移植,采用阿仑单抗诱导、每月一次贝拉西普和每日一次西罗莫司。患者按1:1随机分组接受未分级的供体骨髓。1年后,允许患者停用西罗莫司。对患者进行临床随访并进行监测活检。20例患者接受了移植,均成功。在12个月和36个月时,平均肌酐(估计肾小球滤过率)分别为1.10±0.07mg/dL(89±3.56mL/min)和1.13±0.07mg/dL(88±3.48mL/min)。无论是否输注骨髓,均取得了优异的结果。10例患者选择停用口服免疫抑制剂,其中7例在单用贝拉西普治疗时维持无排斥反应。未能成功停用的患者在基于贝拉西普的治疗方案并辅以口服免疫抑制的情况下成功维持治疗。7例患者拒绝停用免疫抑制剂,3例患者因相关医疗状况被拒绝停用;所有患者均维持无排斥反应。在阿仑单抗诱导后使用时,贝拉西普和西罗莫司可有效预防肾移植排斥反应,而无需使用CNIs或类固醇。部分免疫低风险患者可仅通过每月一次静脉注射贝拉西普维持治疗。