Mayaphi Simnikiwe H, Brauer Marieke, Morobadi Daniel M, Mazanderani Ahmad H, Mafuyeka Rendani T, Olorunju Steve A S, Tintinger Gregory R, Stoltz Anton
Department of Medical Virology, University of Pretoria/National Health Laboratory Service - Tshwane Academic Division (NHLS-TAD), Pretoria, South Africa.
Biostatistics unit, Medical Research Council, Pretoria, South Africa.
PLoS One. 2014 Apr 3;9(4):e93702. doi: 10.1371/journal.pone.0093702. eCollection 2014.
Cytomegalovirus (CMV) infection is associated with severe diseases in immunosuppressed patients; however, there is a lack of data for pre-emptive therapy in patients with HIV/AIDS.
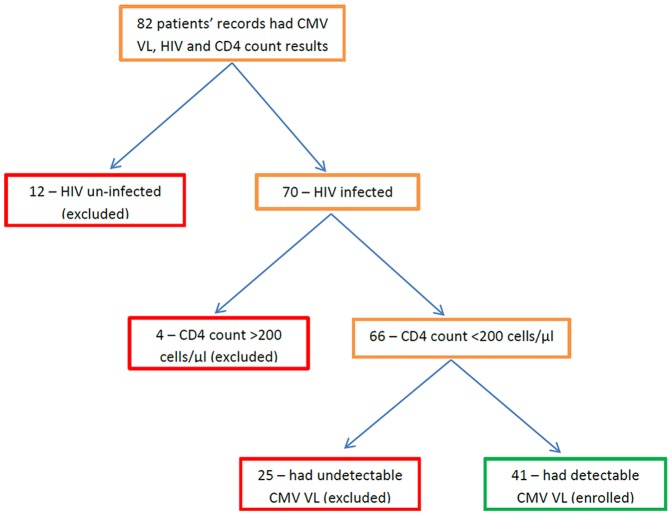
This was a retrospective study, which enrolled patients diagnosed with HIV/AIDS (CD4<200 cells/μl), who had detectable CMV viral load (VL) during their stay in an adult medical intensive care unit between 2009-2012.
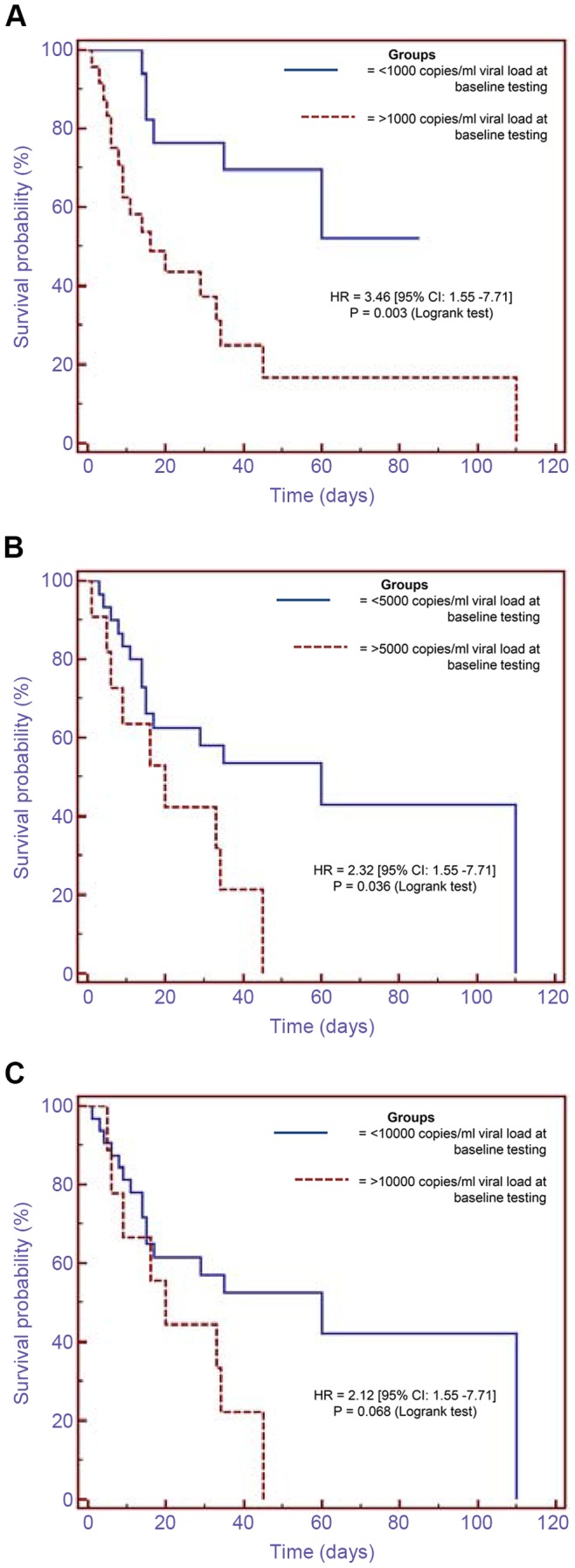
After screening 82 patients' records, 41 patients met the enrolment criteria. Their median age was 37 (interquartile range [IQR]: 31-46), and median CD4 count was 29 cells/μl (IQR: 5-55). Sixteen patients (39%) had serial measurements of CMV VL before treatment with ganciclovir. Patients whose baseline CMV VL values were between 1,000-3,000 copies/ml had significantly higher values (median of 14,650 copies/ml) on follow-up testing done 4-12 days later. Those with undetectable VLs at baseline testing had detectable VLs (median of 1,590 copies/ml) mostly within 20 days of follow-up testing. Patients who had VLs >1,000 copies/ml at baseline testing had significantly higher mortality compared to those who had <1,000 copies/ml {hazard ratio of 3.46, p = 0.003 [95% confidence interval (CI): 1.55-7.71]}. Analysis of the highest CMV VL per patient showed that patients who had VLs of >5,100 copies/ml and did not receive ganciclovir had 100% mortality compared to 58% mortality in those who received ganciclovir at VLs of >5,100 copies/ml, 50% mortality in those who were not treated and had low VLs of <5,100 copies/ml, and 44% mortality in those who had ganciclovir treatment at VLs of <5,100 copies/ml (p = 0.084, 0.046, 0.037, respectively).
This study showed a significantly increased mortality in patients with HIV/AIDS who had high CMV VLs, and suggests that a threshold value of 1,000 copies/ml may be appropriate for pre-emptive treatment in this group.
巨细胞病毒(CMV)感染与免疫抑制患者的严重疾病相关;然而,缺乏关于HIV/AIDS患者进行抢先治疗的数据。
这是一项回顾性研究,纳入了2009年至2012年间在成人医学重症监护病房住院期间被诊断为HIV/AIDS(CD4<200个细胞/μl)且CMV病毒载量(VL)可检测到的患者。
在筛查了82例患者的记录后,41例患者符合纳入标准。他们的中位年龄为37岁(四分位间距[IQR]:31 - 46),中位CD4计数为29个细胞/μl(IQR:5 - 55)。16例患者(39%)在接受更昔洛韦治疗前进行了CMV VL的系列测量。基线CMV VL值在1000 - 3000拷贝/ml之间的患者在4 - 12天后进行的随访检测中其值显著更高(中位值为14,650拷贝/ml)。基线检测时VL不可检测的患者在随访检测后大多在20天内VL变得可检测(中位值为1590拷贝/ml)。基线检测时VL>1000拷贝/ml的患者与VL<1000拷贝/ml的患者相比死亡率显著更高{风险比为3.46,p = 0.003[95%置信区间(CI):1.55 - 7.71]}。对每位患者最高CMV VL的分析表明,VL>5100拷贝/ml且未接受更昔洛韦治疗的患者死亡率为100%,而VL>5100拷贝/ml接受更昔洛韦治疗的患者死亡率为58%,未治疗且VL<5100拷贝/ml较低的患者死亡率为50%,VL<5100拷贝/ml接受更昔洛韦治疗的患者死亡率为44%(p分别为0.084、0.046、0.037)。
本研究表明CMV VL高的HIV/AIDS患者死亡率显著增加,并提示1000拷贝/ml的阈值可能适用于该组患者的抢先治疗。