Sasikumar Deepa, Sasidharan Bijulal, Tharakan Jaganmohan A, Dharan Baiju S, Mathew Thomas, Karunakaran Jayakumar
Departments of Cardiology and Cardiothoracic Surgery, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India.
Ann Pediatr Cardiol. 2014 Jan;7(1):5-12. doi: 10.4103/0974-2069.126538.
Repair of tetralogy of Fallot (TOF) with monocusp pulmonary valve reconstruction prevents pulmonary regurgitation (PR) for a variable period. Since postoperative outcome is governed by PR and right ventricular function, we sought to assess the severity of pulmonary regurgitation and right ventricular outflow (RVOT) gradient in the immediate postoperative period and at 1 year and attempted to identify the anatomical substrates responsible for adverse outcomes.
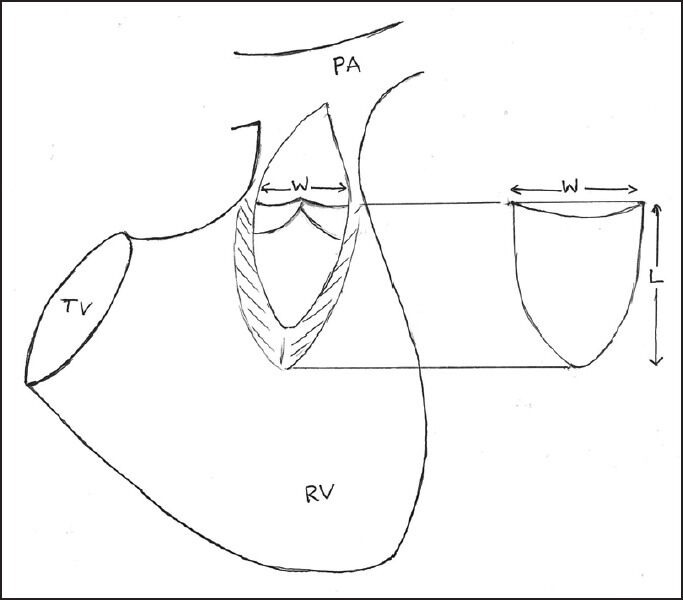
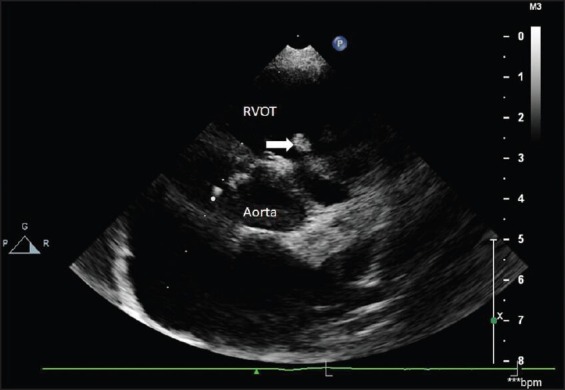
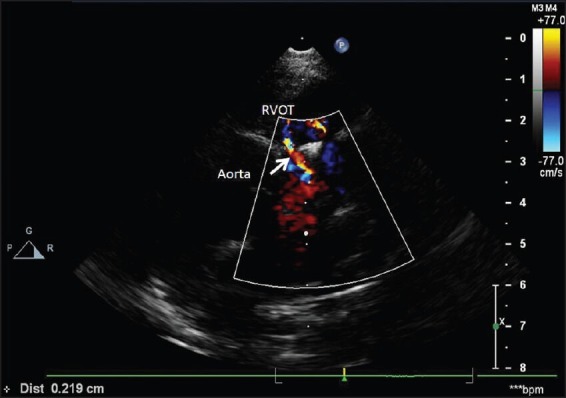
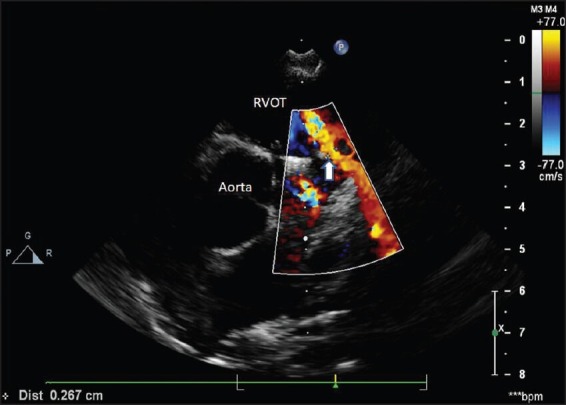
The study included 30 patients. Transthoracic echocardiography was performed before surgery, within 5 days of surgery, and 1 year later. Presence and severity of PR, RVOT gradient, and residual branch pulmonary stenosis were assessed. Right ventricular and monocusp valve functions were studied.
Median age was 36.5 months (3-444 months). There were no deaths. Pulmonary regurgitation was mild in 18, moderate in 10, and severe in 2 patients immediately following surgery. At 1 year, 10 patients had severe PR and one had significant RVOT gradient. None of the variables like age, presence of supravalvar pulmonary branch stenosis, main pulmonary artery diameter, or mobility of monocusp valve was found to have any significant association with the progression of PR. McGoon index <1.5 showed a trend toward more PR, while patients with more residual RVOT gradient had lesser regurgitation.
Repair of TOF with monocusp pulmonary valve reduces immediate postoperative PR. At 1 year, the monocusp valve underwent loss of function in a significant proportion and PR also progressed. This study could not identify any predictors of progression of PR, though patients with McGoon index <1.5 tended to have more PR while those with more outflow gradient had lesser PR.
采用单叶肺动脉瓣重建术修复法洛四联症(TOF)可在一段可变时期内预防肺动脉反流(PR)。由于术后结果受PR和右心室功能影响,我们试图评估术后即刻、1年时肺动脉反流的严重程度及右心室流出道(RVOT)梯度,并试图确定导致不良结局的解剖学基础。
本研究纳入30例患者。在手术前、术后5天内及1年后进行经胸超声心动图检查。评估PR的存在及严重程度、RVOT梯度和残余分支肺动脉狭窄情况。研究右心室和单叶瓣膜功能。
中位年龄为36.5个月(3 - 444个月)。无死亡病例。术后即刻,18例患者PR为轻度,10例为中度,2例为重度。1年时,10例患者有重度PR,1例有明显RVOT梯度。未发现年龄、肺动脉瓣上分支狭窄的存在、主肺动脉直径或单叶瓣膜活动度等变量与PR进展有任何显著关联。McGoon指数<1.5显示出PR更多的趋势,而RVOT残余梯度更大的患者反流较少。
采用单叶肺动脉瓣修复TOF可降低术后即刻PR。1年时,相当比例的单叶瓣膜功能丧失,PR也有所进展。本研究未能确定PR进展的任何预测因素,尽管McGoon指数<1.5的患者PR往往更多,而流出道梯度更大的患者PR较少。