Lung Infection and Immunity Unit, Division of Pulmonology & UCT Lung Institute, Department of Medicine, University of Cape Town, Cape Town, South Africa.
BMC Pulm Med. 2014 Apr 8;14:58. doi: 10.1186/1471-2466-14-58.
The accuracy of currently available same-day diagnostic tools (smear microscopy and conventional nucleic acid amplification tests) for pleural tuberculosis (TB) is sub-optimal. Newer technologies may offer improved detection.
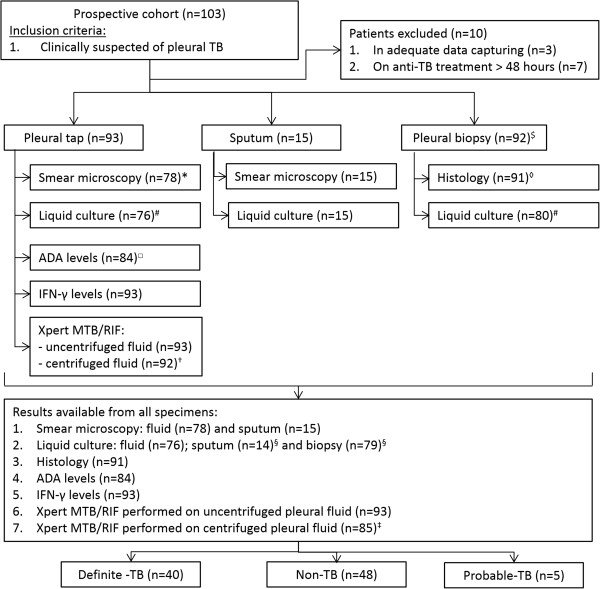
Smear-microscopy, adenosine deaminase (ADA), interferon gamma (IFN-γ), and Xpert MTB/RIF [using an unprocessed (1 ml) and centrifuged (~20 ml) sample] test accuracy was evaluated in pleural fluid from 103 consecutive patients with suspected pleural TB. Culture for M.tuberculosis and/or histopathology (pleural biopsy) served as the reference standard. Patients were followed prospectively to determine their diagnostic categorisation.
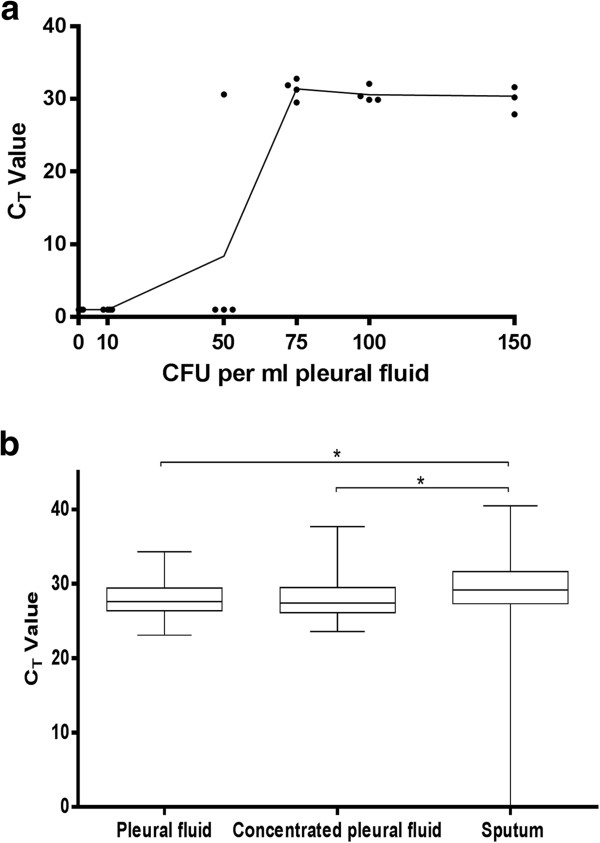
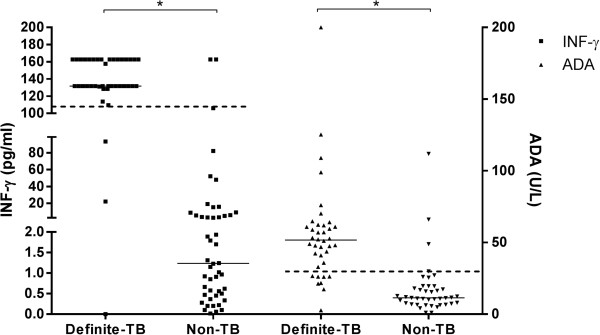
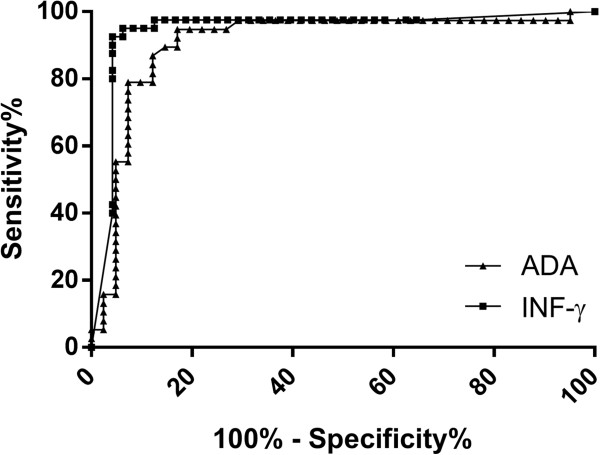
Of 93 evaluable participants, 40 had definite-TB (reference positive), 5 probable-TB (not definite but treated for TB) and 48 non-TB (culture and histology negative, and not treated for TB). Xpert MTB/RIF sensitivity and specificity (95% CI) was 22.5% (12.4 - 37.6) and 98% (89.2 - 99.7), respectively, and centrifugation did not improve sensitivity (23.7%). The Xpert MTB/RIF internal positive control showed no evidence of inhibition. Biomarker specific sensitivity, specificity, PPV, and NPVs were: ADA (48.85 IU/L; rule-in cut-point) 55.3% (39.8 - 69.9), 95.2% (83.9 - 98.7), 91.4 (73.4 - 95.4), 69.7% (56.7 - 80.1); ADA (30 IU/L; clinically used cut-point) 79% (63.7 - 89), 92.7% (80.6 - 97.5), 91.0 (73.4 - 95.4), 82.7% (69.3 - 90.1); and IFN-γ (107.7 pg/ml; rule-in cut-point) 92.5% (80.2 - 97.5), 95.9% (86.1 - 98.9), 94.9% (83.2 - 98.6), 93.9% (83.5 - 97.9), respectively (IFN-γ sensitivity and NPV better than Xpert [p < 0.05] and rule-in ADA [p < 0.05]).
The usefulness of Xpert MTB/RIF to diagnose pleural TB is limited by its poor sensitivity. IFN-γ is an excellent rule-in test and, compared to ADA, has significantly better sensitivity and rule-out value in a TB-endemic setting.
目前用于胸腔结核(TB)的即时诊断工具(涂片显微镜检查和常规核酸扩增试验)的准确性不理想。新技术可能会提供更好的检测。
在 103 例疑似胸腔 TB 患者的胸腔积液中评估了涂片显微镜检查、腺苷脱氨酶(ADA)、干扰素γ(IFN-γ)和 Xpert MTB/RIF [使用未经处理(1ml)和离心(~20ml)样本] 的检测准确性。分枝杆菌培养和/或组织病理学(胸腔活检)作为参考标准。对患者进行前瞻性随访以确定其诊断分类。
在 93 例可评估的参与者中,40 例为明确-TB(参考阳性),5 例为可能-TB(不明确但接受 TB 治疗),48 例为非-TB(培养和组织学阴性,且未接受 TB 治疗)。Xpert MTB/RIF 的敏感性和特异性(95%CI)分别为 22.5%(12.4-37.6)和 98%(89.2-99.7),离心处理并未提高敏感性(23.7%)。Xpert MTB/RIF 内部阳性对照未显示出抑制迹象。生物标志物的特异性敏感性、特异性、PPV 和 NPV 分别为:ADA(48.85IU/L;规则内切点)55.3%(39.8-69.9)、95.2%(83.9-98.7)、91.4%(73.4-95.4)、69.7%(56.7-80.1);ADA(30IU/L;临床使用切点)79%(63.7-89)、92.7%(80.6-97.5)、91.0%(73.4-95.4)、82.7%(69.3-90.1);IFN-γ(107.7pg/ml;规则内切点)92.5%(80.2-97.5)、95.9%(86.1-98.9)、94.9%(83.2-98.6)、93.9%(83.5-97.9)(IFN-γ的敏感性和 NPV 优于 Xpert [p<0.05]和规则内 ADA [p<0.05])。
Xpert MTB/RIF 诊断胸腔结核的有效性受到其敏感性差的限制。IFN-γ是一种优秀的规则内检测方法,与 ADA 相比,在结核病流行地区具有更好的敏感性和排除价值。