Department of Conflict Resolution, Human Security & Global Governance; and College of Nursing and Health Sciences, University of Massachusetts Boston, 100 Morrissey Blvd, Boston, MA 02125, USA.
Int J Equity Health. 2014 Apr 8;13:28. doi: 10.1186/1475-9276-13-28.
In a significant geographical shift in the distribution of HIV infection, the US South--comprising 17 states--now has the greatest number of adults and adolescents with HIV (PLHIV) in the nation. More than 60% of PLHIV are not in HIV care in Alabama and Mississippi, contrasted with a national figure of 25%. Poorer HIV outcomes raise concerns about HIV-related inequities for southern PLHIV, which warrant further study. This qualitative study sought to understand experiences of low-income PLHIV on the AIDS Drug Assistance Program in engagement and retention in continuous HIV care in two sites in Alabama.
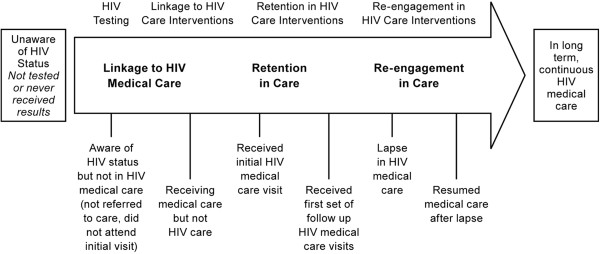
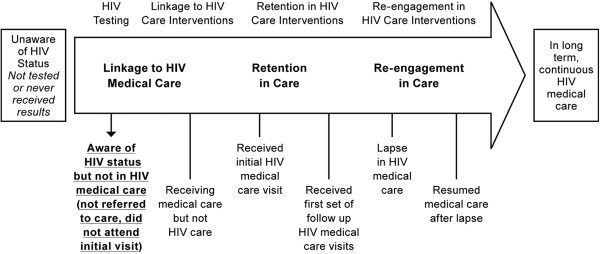
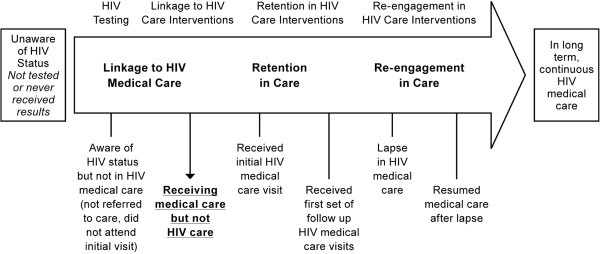
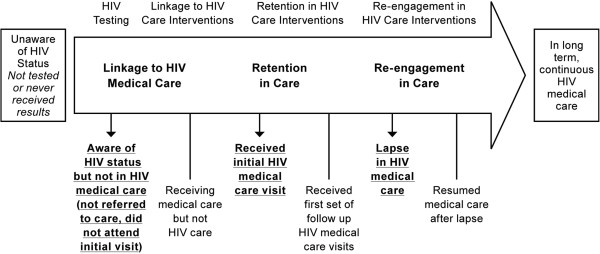
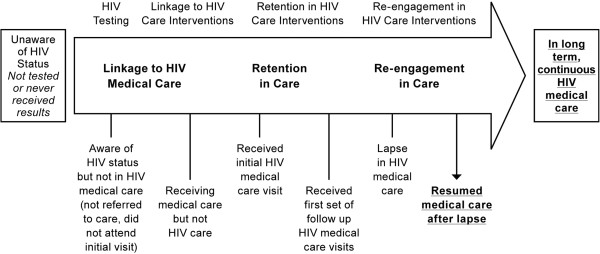
The study was designed using grounded theory. Semi-structured interviews with 25 PLHIV explored experiences with care linkage, reported factors and behaviors affecting engagement/retention in continuous HIV care, including socio-economic factors. To triangulate sources, 25 additional interviews were conducted with health and social service providers from the same clinics and AIDS Service Organizations where clients obtained services. Across the narratives, we used the HIV care continuum to map where care delays and drop out occurred. Using open coding, constant comparison and iterative data collection and analysis, we constructed a conceptual model illustrating how participants described their path to HIV care engagement and retention.
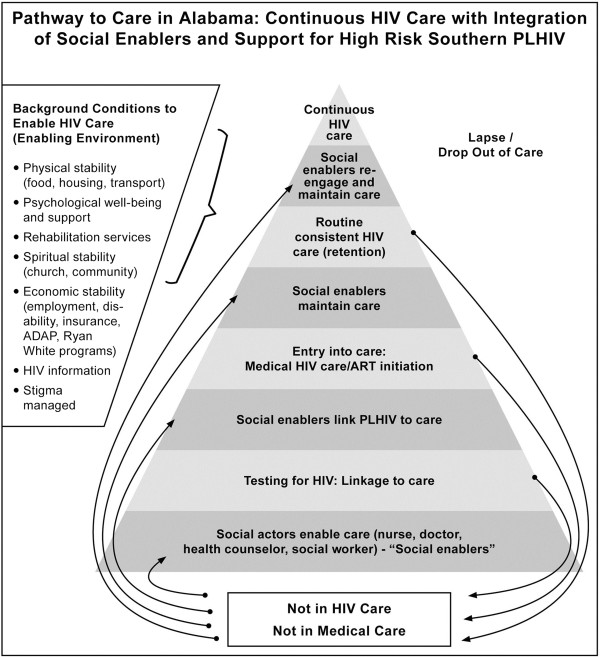
Most respondents reported delayed HIV care, describing concentric factors: psychological distress, fear, lack of information, substance use, incarceration, lack of food, transport and housing. Stark health system drop out occurred immediately after receipt of HIV test results, with ART initiation generally occurring when individuals became ill. Findings highlight these enablers to care: Alabama's 'social infrastructure'; 'twinning' medical with social services, 'social enablers' who actively link PLHIV to care; and 'enabling spaces' that break down PLHIV isolation, facilitating HIV care linkage/retention.
Ryan White-funded programs, together with housing, food and psychological support were pre-conditions for participants' entry and retention in HIV care. The path to achieving continuous HIV care for individuals at risk of lack of entry or delayed HIV care requires robust social-level responses, like in Alabama, that address physical and mental health of clients and directly engage the particular social and economic contexts and vulnerabilities of southern PLHIV.
随着艾滋病毒感染的分布在地理上发生重大转变,美国南部(包括 17 个州)现在拥有全国最多的成年和青少年艾滋病毒感染者(PLHIV)。阿拉巴马州和密西西比州有超过 60%的 PLHIV 没有接受艾滋病毒护理,而全国这一比例为 25%。较差的艾滋病毒结果引发了对美国南部 PLHIV 艾滋病毒相关不平等问题的担忧,这需要进一步研究。这项定性研究旨在了解阿拉巴马州两个地点的艾滋病药物援助计划中低收入 PLHIV 在参与和持续接受艾滋病毒护理方面的经历。
该研究采用扎根理论设计。对 25 名 PLHIV 进行了半结构化访谈,探讨了他们在获得护理方面的经验,报告了影响他们持续接受艾滋病毒护理的因素和行为,包括社会经济因素。为了对信息进行三角验证,还对来自同一诊所和 AIDS 服务组织的 25 名额外卫生和社会服务提供者进行了访谈,这些诊所和 AIDS 服务组织是客户获得服务的地方。在整个叙述中,我们使用艾滋病毒护理连续体来映射护理延迟和退出的位置。通过开放编码、不断比较和迭代数据收集和分析,我们构建了一个概念模型,说明参与者如何描述他们参与和维持艾滋病毒护理的途径。
大多数受访者报告说,他们的艾滋病毒护理出现了延迟,描述了同心因素:心理困扰、恐惧、缺乏信息、药物滥用、监禁、缺乏食物、交通和住房。当他们收到艾滋病毒检测结果后,患者立即离开了卫生系统,而当他们生病时,他们才开始接受抗逆转录病毒治疗。研究结果强调了这些促进护理的因素:阿拉巴马州的“社会基础设施”;将医疗与社会服务“配对”,积极将 PLHIV 与护理联系起来的“社会促进者”;以及打破 PLHIV 孤立的“促进空间”,促进 HIV 护理的联系/保留。
受 Ryan White 资助的项目,以及住房、食品和心理支持,是参与者进入和维持艾滋病毒护理的前提条件。对于那些有缺乏进入或延迟艾滋病毒护理风险的个人,实现持续艾滋病毒护理的途径需要强有力的社会层面的反应,就像在阿拉巴马州一样,这需要解决客户的身心健康问题,并直接参与到南部 PLHIV 的特殊社会和经济背景和脆弱性中。