Lin Chih-Hung, Kang Chung-Jan, Tsao Chung-Kan, Wallace Christopher Glenn, Lee Li-Yu, Lin Chien-Yu, Wang Hung-Ming, Ng Shu-Hang, Yen Tzu-Chen, Liao Chun-Ta
Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan, R.O.C.; Department of Head and Neck Oncology Group, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan, R.O.C.
Department of Head and Neck Oncology Group, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan, R.O.C.; Department of Otorhinolaryngology, Head and Neck Surgery, Chang Gung Memorial Hospital and Chang Gung University, Taoyuan, Taiwan, R.O.C.
PLoS One. 2014 Apr 10;9(4):e94315. doi: 10.1371/journal.pone.0094315. eCollection 2014.
The fibula osteoseptocutaneous free flap is generally used for segmental mandibular reconstructions following resection of oral cavity squamous cell carcinoma (OSCC). However, less complex reconstructions may be feasible for patients with predicted poor survival. Herein, we sought to identify the main risk factors (RFs) associated with poor prognosis in OSCC patients undergoing segmental mandibulectomy to help decide between fibular and non-fibular reconstructions.
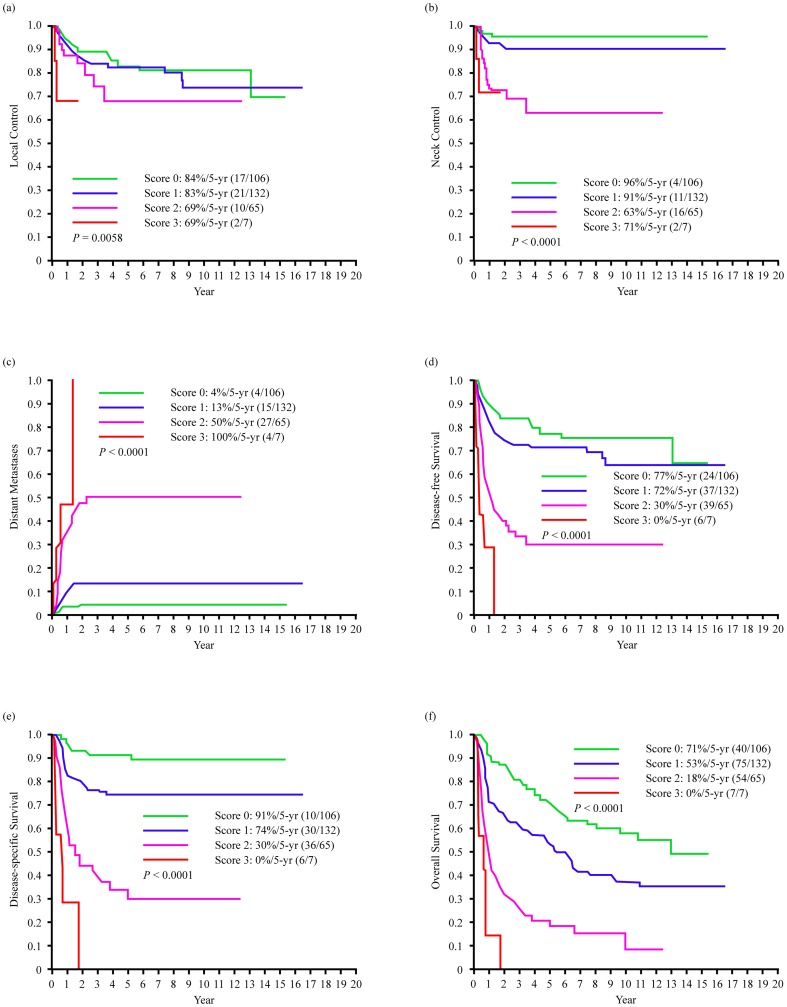
Between 1996 and 2011, we examined the 5-year control, distant metastases, and survival rates in 310 consecutive, previously untreated patients with primary OSCC who underwent segmental mandibulectomy.
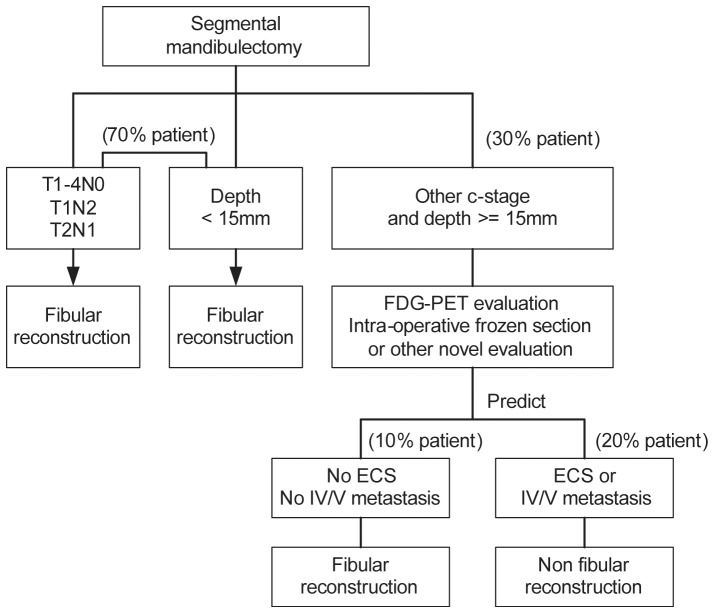
Margin status was the only independent RF for 5-year local control. Level IV/V metastases, extracapsular spread, and tumor depth ≥15 mm were independent RFs for poor 5-year survival. In the entire study cohort, 23% of the patients had 2 or 3 adverse RFs; such a high-risk group was characterized by a poor prognosis and may be suitable for non-fibular reconstructions. Overall, 70% of the study patients were cT1-4N0, cT1N2, cT2N1, or had tumor depth <15 mm; less than 5% of patients in this subgroup had 2 or 3 adverse RFs and were thus candidates for fibular reconstructions. Among the remaining 30% of patients who showed both advanced clinical stage (cT2N2, cT3-4N1-2) and tumor depth ≥15 mm, 70% exhibited 2 or 3 adverse RFs.
Level IV/V metastases, extracapsular spread, and tumor depth ≥15 mm were independent predictors of poor prognosis in OSCC patients undergoing segmental mandibulectomy. The preoperative or intraoperative identification of adverse RFs may help decide between fibular and non-fibular mandibular reconstruction. High-risk patients bearing 2 or 3 adverse RFs have poor prognosis and should not be considered as candidates for fibular reconstructions.
腓骨骨-皮-肌瓣游离皮瓣通常用于口腔鳞状细胞癌(OSCC)切除术后的下颌骨节段性重建。然而,对于预计生存期较短的患者,采用不太复杂的重建方式可能是可行的。在此,我们试图确定接受下颌骨节段切除术的OSCC患者预后不良的主要危险因素(RFs),以帮助决定采用腓骨重建还是非腓骨重建。
在1996年至2011年期间,我们对310例连续的、未经治疗的原发性OSCC患者进行了研究,这些患者均接受了下颌骨节段切除术,并对其5年局部控制率、远处转移率和生存率进行了评估。
切缘状态是5年局部控制的唯一独立危险因素。IV/V级转移、包膜外扩散和肿瘤深度≥15 mm是5年生存率低的独立危险因素。在整个研究队列中,23%的患者有2个或3个不良危险因素;这样的高危组预后较差,可能适合非腓骨重建。总体而言,70%的研究患者为cT1-4N0、cT1N2、cT2N1,或肿瘤深度<15 mm;该亚组中不到5%的患者有2个或3个不良危险因素,因此是腓骨重建的候选者。在其余30%临床分期较晚(cT2N2、cT3-4N1-2)且肿瘤深度≥15 mm的患者中,70%有2个或3个不良危险因素。
IV/V级转移、包膜外扩散和肿瘤深度≥15 mm是接受下颌骨节段切除术的OSCC患者预后不良的独立预测因素。术前或术中识别不良危险因素可能有助于决定采用腓骨还是非腓骨下颌骨重建。有2个或3个不良危险因素的高危患者预后较差,不应被视为腓骨重建的候选者。