Kong Seom Gim, Seo Jung Ho, Jun So Eun, Lee Byung Ki, Lim Young Tak
Department of Pediatrics, Pusan National University College of Medicine, Busan, Korea.
Blood Res. 2014 Mar;49(1):29-35. doi: 10.5045/br.2014.49.1.29. Epub 2014 Mar 24.
Hyperleukocytosis caused by acute lymphoblastic leukemia (ALL) is associated with early morbidity and mortality due to hyperviscosity arising from the excessive number of leukocytes.This study was designed to assess the incidence of hyperleukocytosis, survival outcomes, and adverse features among pediatric ALL patients with hyperleukocytosis.
Between January 2001 and December 2010, 104 children with previously untreated ALL were enrolled at the Pusan National University Hospital. All of them were initially stratified based on the National Cancer Institute (NCI) risk; 48 (46.2%) were diagnosed with high-risk ALL. The medical charts of these patients were retrospectively reviewed.
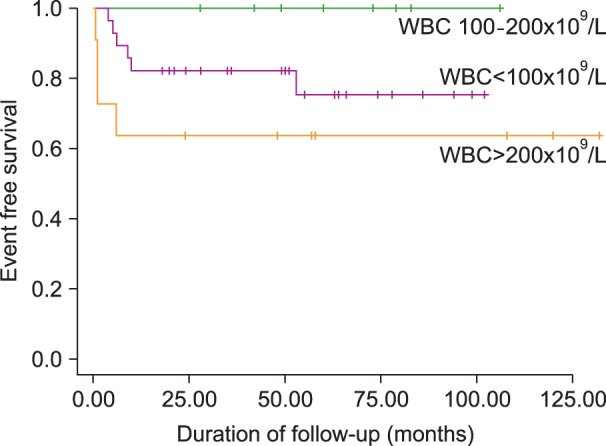
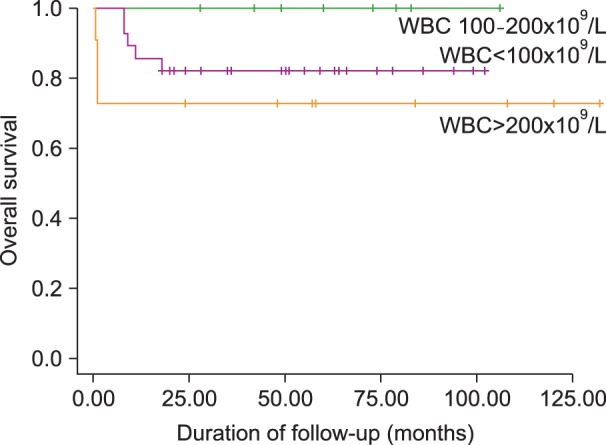
Twenty (19.2%) of the 104 children with ALL had initial leukocyte counts of >100×10(9)/L, and 11 patients had a leukocyte count of >200×10(9)/L. Male gender, T-cell phenotype, and massive splenomegaly were positively associated with hyperleukocytosis. Common early complications during induction therapy included renal dysfunction, and central nervous system hemorrhage. The complete remission (CR) rate for the pediatric ALL patients with hyperleukocytosis (94.1%) was similar to the overall CR rate (95.6%). The estimated 3-year event free survival (EFS) and overall survival of ALL children with hyperleukocytosis were 75.0% and 81.2%, respectively. However, patients with initial leukocyte counts >200×10(9)/L had a lower EFS than those with initial leukocyte counts 100-200×10(9)/L (63.6% vs. 100%; P=0.046).
The outcome of pediatric ALL cases with an initial leukocyte count >200×10(9)/L was very poor, probably due to early toxicity-related death during induction therapy.
急性淋巴细胞白血病(ALL)引起的白细胞增多症与因白细胞数量过多导致的血液高黏滞度相关的早期发病和死亡有关。本研究旨在评估小儿ALL合并白细胞增多症患者中白细胞增多症的发生率、生存结局及不良特征。
2001年1月至2010年12月期间,104例既往未接受治疗的ALL患儿在釜山国立大学医院入组。所有患儿最初均根据美国国立癌症研究所(NCI)风险进行分层;48例(46.2%)被诊断为高危ALL。对这些患者的病历进行回顾性分析。
104例ALL患儿中有20例(19.2%)初始白细胞计数>100×10⁹/L,11例患者白细胞计数>200×10⁹/L。男性、T细胞表型和巨脾与白细胞增多症呈正相关。诱导治疗期间常见的早期并发症包括肾功能不全和中枢神经系统出血。小儿ALL合并白细胞增多症患者的完全缓解(CR)率(94.1%)与总体CR率(95.6%)相似。小儿ALL合并白细胞增多症患儿的3年无事件生存率(EFS)和总生存率分别为75.0%和81.2%。然而,初始白细胞计数>200×10⁹/L的患者的EFS低于初始白细胞计数为100 - 200×10⁹/L的患者(63.6%对100%;P = 0.046)。
初始白细胞计数>200×10⁹/L的小儿ALL病例结局非常差,可能是由于诱导治疗期间与毒性相关的早期死亡。