Pastore Friederike, Pastore Alessandro, Wittmann Georg, Hiddemann Wolfgang, Spiekermann Karsten
Department of Internal Medicine III, University Hospital Munich, Ludwig-Maximilians-University Munich - Campus Groβhadern, Munich, Germany; German Cancer Consortium (DKTK), Heidelberg, Germany; German Cancer Research Center (DKFZ), Heidelberg, Germany.
Department of Internal Medicine III, University Hospital Munich, Ludwig-Maximilians-University Munich - Campus Groβhadern, Munich, Germany.
PLoS One. 2014 Apr 14;9(4):e95062. doi: 10.1371/journal.pone.0095062. eCollection 2014.
Hyperleukocytosis in AML with leukostasis is a serious life-threatening condition leading to a high early mortality which requires immediate cytoreductive therapy. Therapeutic leukapheresis is currently recommended by the American Society of Apheresis in patients with a WBC>100 G/l with signs of leukostasis, but the role of prophylactic leukapheresis before clinical signs of leukostasis occur is unclear.
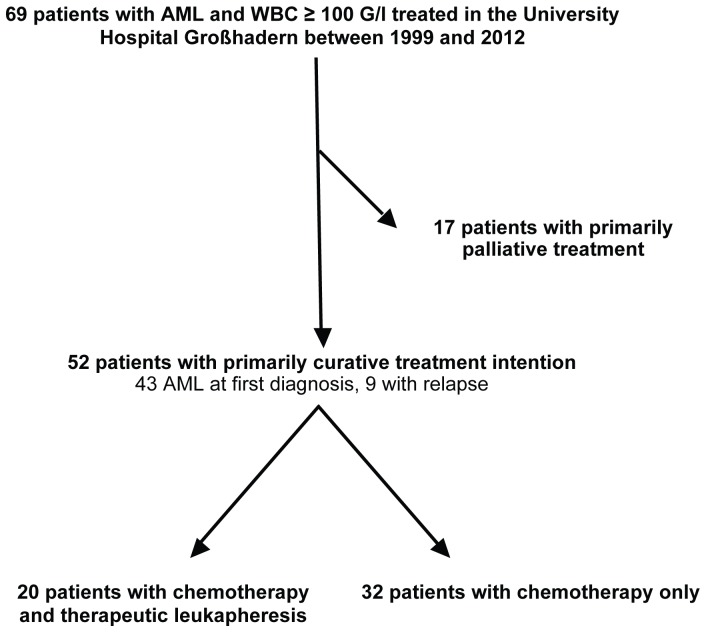
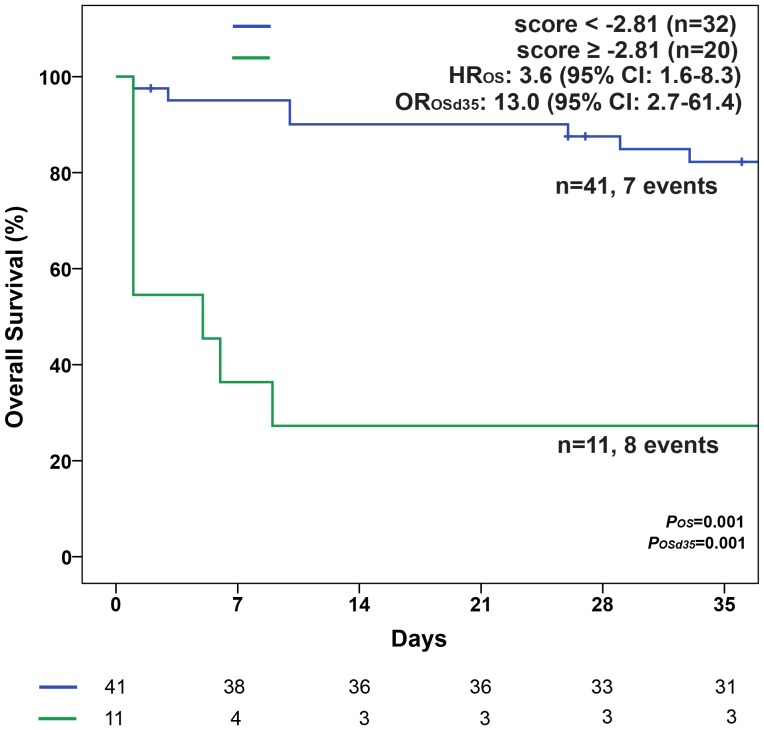
We retrospectively analyzed the role of leukapheresis in 52 patients (median age 60 years) with hyperleukocytotic AML with and without clinical signs of leukostasis. Since leukapheresis was performed more frequently in patients with signs of leukostasis due to the therapeutic policy in our hospital, we developed a risk score for early death within seven days after start of therapy (EDd7) to account for this selection bias and to independently measure the effect of leukapheresis on EDd7.
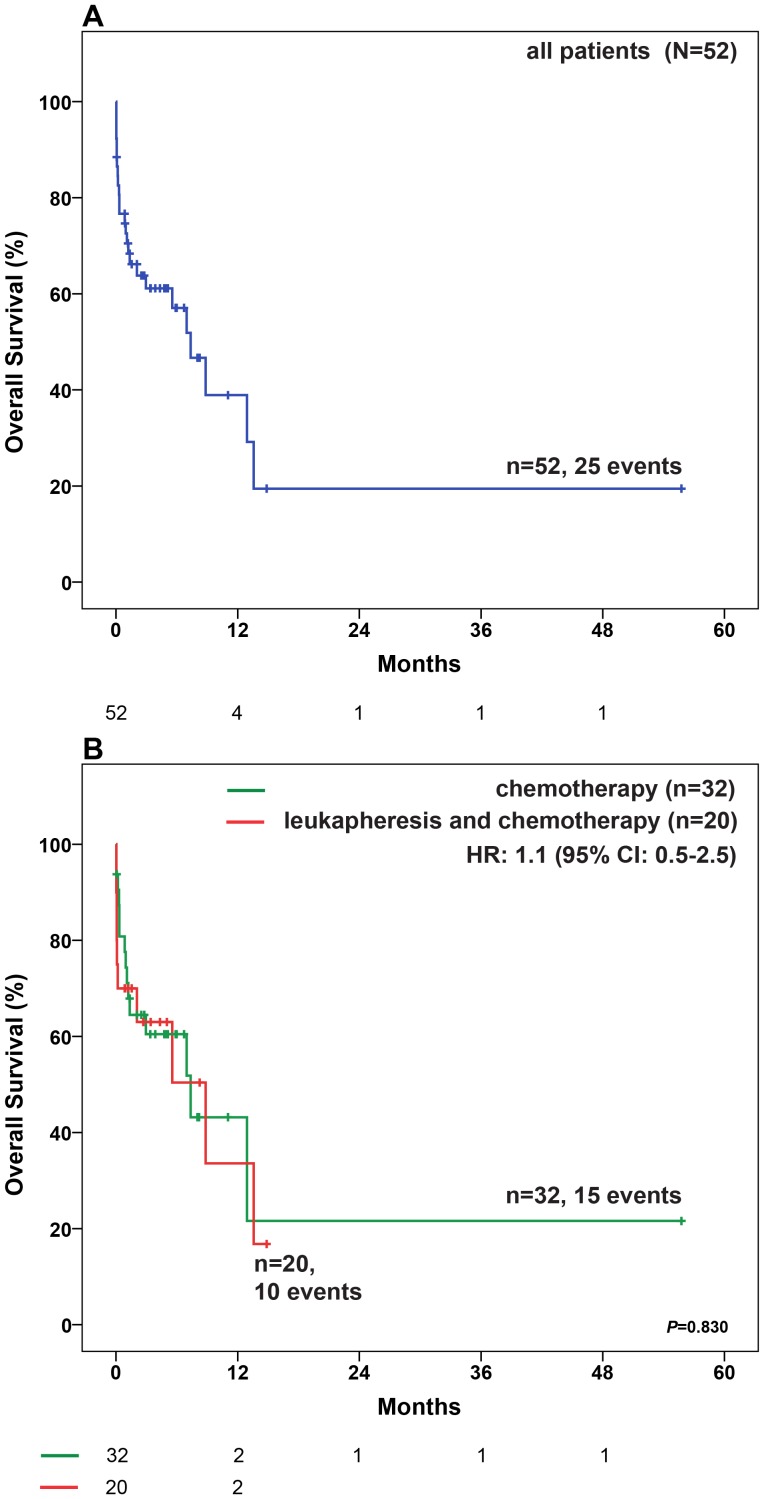
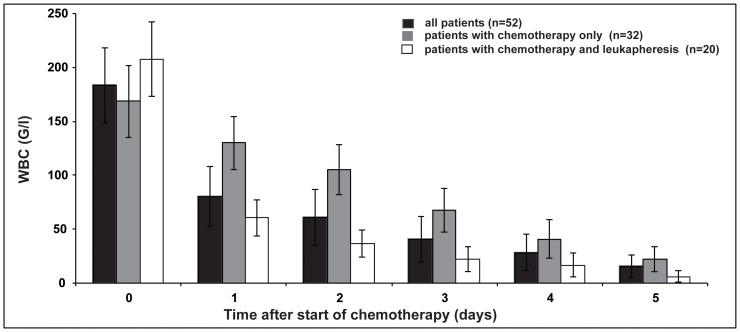
20 patients received leukapheresis in combination to chemotherapy compared to 32 patients who received chemotherapy only. In a multivariate logistic regression model for the estimation of the probability of EDd7 thromboplastin time and creatinine remained as independent significant parameters and were combined to create an EDd7 risk score. The effect of leukapheresis on EDd7 was evaluated in a bivariate logistic regression together with the risk score. Leukapheresis did not significantly change early mortality in all patients with a WBC≥100 G/l.
Prophylactic leukapheresis in hyperleukocytotic patients with and without leukostasis did not improve early mortality in our retrospective study. Larger and prospective clinical trials are needed to validate the risk score and to further explore the role of leukapheresis in AML with hyperleukocytosis.
急性髓系白血病(AML)合并白细胞淤滞的高白细胞血症是一种严重的危及生命的状况,会导致较高的早期死亡率,需要立即进行细胞减灭治疗。美国单采学会目前推荐对白细胞计数>100×10⁹/L且有白细胞淤滞体征的患者进行治疗性白细胞单采,但在白细胞淤滞临床体征出现之前进行预防性白细胞单采的作用尚不清楚。
我们回顾性分析了52例(中位年龄60岁)有或无白细胞淤滞临床体征的高白细胞性AML患者白细胞单采的作用。由于我院的治疗策略,有白细胞淤滞体征的患者更频繁地接受白细胞单采,我们制定了一个治疗开始后7天内早期死亡(EDd7)的风险评分来解释这种选择偏倚,并独立测量白细胞单采对EDd7的影响。
20例患者接受白细胞单采联合化疗,32例患者仅接受化疗。在用于估计EDd7概率的多变量逻辑回归模型中,凝血酶原时间和肌酐仍然是独立的显著参数,并将其合并以创建EDd7风险评分。在双变量逻辑回归中结合风险评分评估白细胞单采对EDd7的影响。白细胞单采并未显著改变所有白细胞≥100×10⁹/L患者的早期死亡率。
在我们的回顾性研究中,有或无白细胞淤滞的高白细胞血症患者进行预防性白细胞单采并未改善早期死亡率。需要更大规模的前瞻性临床试验来验证风险评分,并进一步探索白细胞单采在高白细胞性AML中的作用。