Voscopoulos Christopher, Ladd Diane, Campana Lisa, George Edward
Department of Anesthesiology, Perioperative and Pain Medicine, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
School of Nursing, West Virginia University, Morgantown WV, USA ; Respiratory Motion, Inc., Waltham MA, USA.
J Clin Med Res. 2014 Jun;6(3):209-14. doi: 10.14740/jocmr1718w. Epub 2014 Mar 31.
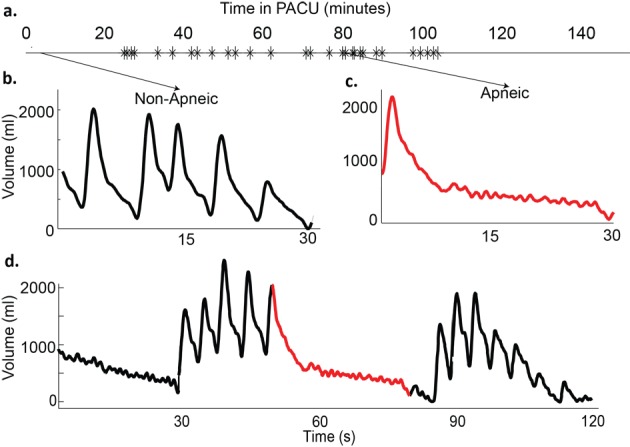
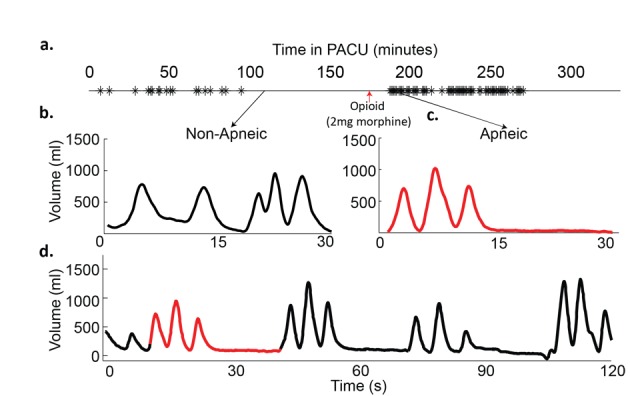
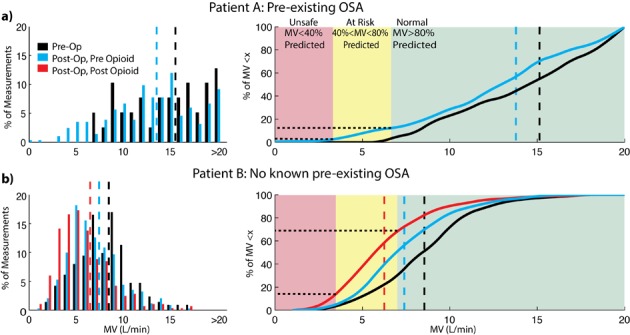
Obstructive sleep apnea (OSA) is a potential independent risk factor for postoperative complications, adverse surgical outcomes, and longer hospital stays. Obese patients with OSA have increased post-operative complications. An estimated 25-30% of pre-operative patients are at a high risk for OSA. A novel, non-invasive respiratory volume monitor (RVM) has been developed to provide a real time respiratory curve demonstrating lung volumes as well as a continuous, display of minute ventilation, tidal volume and respiratory rate. Clinical application of this device in the post-anesthesia care unit (PACU) can "unmask" post-operative apneic events resulting from partial or complete airway collapse due to the residual effects of narcotic administration and volatile and/or intravenous anesthetics. Clinical examples from two patients, one with known OSA and one without a previous diagnosis of OSA, monitored in the PACU with RVM are presented here. Post-operatively both patients had an increase in apneic episodes with significant decreases in their MV during apneic episodes after opioid administration as compared to pre-op baseline. In addition, oxygen saturation, for both patients, which is an essential component of current respiratory monitoring remained normal in the cases presented, despite the significant decreases in MV. Continuous RVM monitoring demonstrates both changes in respiratory patterns and overall adequacy of ventilation, and allows practitioners to quantify the increase in the number and duration apneic episodes as a response to narcotic administration. These case studies demonstrate that a non-invasive respiratory volume monitoring system can detect and quantify respiratory disturbances that currently go undetected.
阻塞性睡眠呼吸暂停(OSA)是术后并发症、不良手术结局及更长住院时间的潜在独立危险因素。患有OSA的肥胖患者术后并发症增多。估计25% - 30%的术前患者存在OSA高风险。一种新型非侵入性呼吸容积监测仪(RVM)已研发出来,可提供实时呼吸曲线以显示肺容积,并持续显示分钟通气量、潮气量和呼吸频率。该设备在麻醉后护理单元(PACU)的临床应用能够“揭示”因麻醉剂、挥发性和/或静脉麻醉剂的残留作用导致部分或完全气道塌陷所引起的术后呼吸暂停事件。本文展示了在PACU使用RVM监测的两名患者的临床案例,一名已知患有OSA,另一名既往未诊断出OSA。术后,与术前基线相比,两名患者在使用阿片类药物后呼吸暂停发作均增多,且呼吸暂停发作期间分钟通气量显著下降。此外,在本文所呈现的案例中,尽管分钟通气量显著下降,但两名患者的氧饱和度(当前呼吸监测的重要组成部分)均保持正常。持续的RVM监测可显示呼吸模式的变化以及通气的整体充足性,并使从业者能够量化因麻醉剂使用导致的呼吸暂停发作次数和持续时间的增加。这些案例研究表明,一种非侵入性呼吸容积监测系统能够检测和量化目前未被发现的呼吸紊乱情况。