Mehta Jaideep H, Cattano Davide, Brayanov Jordan B, George Edward E
University of Texas Medical School at Houston, 6431 Fannin Street, Houston, TX, 77030, USA.
Respiratory Motion Inc., 411 Waverley Oaks Rd #150, Waltham, MA, 02452, USA.
BMC Anesthesiol. 2017 Apr 26;17(1):61. doi: 10.1186/s12871-017-0352-0.
Monitoring the adequacy of spontaneous breathing is a major patient safety concern in the post-operative setting. Monitoring is particularly important for obese patients, who are at a higher risk for post-surgical respiratory complications and often have increased metabolic demand due to excess weight. Here we used a novel, noninvasive Respiratory Volume Monitor (RVM) to monitor ventilation in both obese and non-obese orthopedic patients throughout their perioperative course, in order to develop better monitoring strategies.
We collected respiratory data from 62 orthopedic patients undergoing elective joint replacement surgery under general anesthesia using a bio-impedance based RVM with an electrode PadSet placed on the thorax. Patients were stratified into obese (BMI ≥ 30) and non-obese cohorts and minute ventilation (MV) at various perioperative time points was compared against each patient's predicted minute ventilation (MV) based on ideal body weight (IBW) and body surface area (BSA). The distributions of MV measurements were also compared across obese and non-obese cohorts.
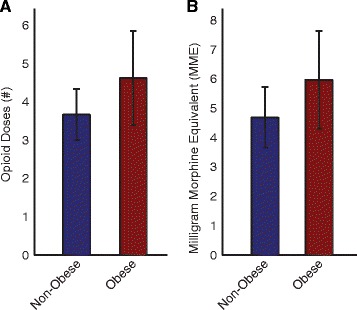
Obese patients had higher MV than the non-obese patients before, during, and after surgery. Measured MV of obese patients was significantly higher than their MV from IBW formulas, with BSA-based MV being a closer estimate. Obese patients also had greater variability in MV post-operatively when treated with standard opioid dosing.
Our study demonstrated that obese patients have greater variability in ventilation post-operatively when treated with standard opioid doses, and despite overall higher ventilation, many of them are still at risk for hypoventilation. BSA-based MV formulas may be more appropriate than IBW-based ones when estimating the respiratory demand of obese patients. The RVM allows for the continuous and non-invasive assessment of respiratory function in both obese and non-obese patients.
在术后环境中,监测自主呼吸是否充分是患者安全的一个主要关注点。监测对于肥胖患者尤为重要,他们术后发生呼吸并发症的风险更高,并且由于体重过重,代谢需求往往增加。在此,我们使用一种新型的非侵入性呼吸容积监测仪(RVM),在肥胖和非肥胖骨科患者的整个围手术期过程中监测通气情况,以便制定更好的监测策略。
我们使用基于生物阻抗的RVM,将电极垫放置在胸部,收集了62例接受全身麻醉下择期关节置换手术的骨科患者的呼吸数据。患者被分为肥胖(BMI≥30)和非肥胖队列,并将各个围手术期时间点的分钟通气量(MV)与基于理想体重(IBW)和体表面积(BSA)的每位患者的预测分钟通气量进行比较。还比较了肥胖和非肥胖队列中MV测量值的分布情况。
肥胖患者在手术前、手术中和手术后的MV均高于非肥胖患者。肥胖患者的实测MV显著高于根据IBW公式计算出的MV,而基于BSA的MV是更接近的估计值。在接受标准阿片类药物剂量治疗时,肥胖患者术后的MV变异性也更大。
我们的研究表明,肥胖患者在接受标准阿片类药物剂量治疗时,术后通气变异性更大,尽管总体通气量较高,但其中许多人仍有通气不足的风险。在估计肥胖患者的呼吸需求时,基于BSA的MV公式可能比基于IBW的公式更合适。RVM能够对肥胖和非肥胖患者的呼吸功能进行连续和非侵入性评估。