Eriksson Jonas K, Karlsson Johan A, Bratt Johan, Petersson Ingemar F, van Vollenhoven Ronald F, Ernestam Sofia, Geborek Pierre, Neovius Martin
Clinical Epidemiology Unit, Department of Medicine, Karolinska Institutet, Stockholm, Sweden.
Section of Rheumatology, Department of Clinical Sciences Lund, Lund University, Lund, Sweden.
Ann Rheum Dis. 2015 Jun;74(6):1094-101. doi: 10.1136/annrheumdis-2013-205060. Epub 2014 Apr 15.
To estimate the incremental cost-effectiveness of infliximab versus conventional combination treatment over 21 months in patients with methotrexate-refractory early rheumatoid arthritis.
In this multicentre, two-arm, parallel, randomised, active-controlled, open-label trial, rheumatoid arthritis patients with <1 year symptom duration were recruited from 15 rheumatology clinics in Sweden between October 2002 and December 2005. After 3-4 months of methotrexate monotherapy, patients not achieving low disease activity were randomised to addition of infliximab or sulfasalazine+hydroxychloroquine (conventional treatment group). Costs of drugs, healthcare use, and productivity losses were retrieved from nationwide registers, while EuroQol 5-Dimensions utility was collected quarterly.
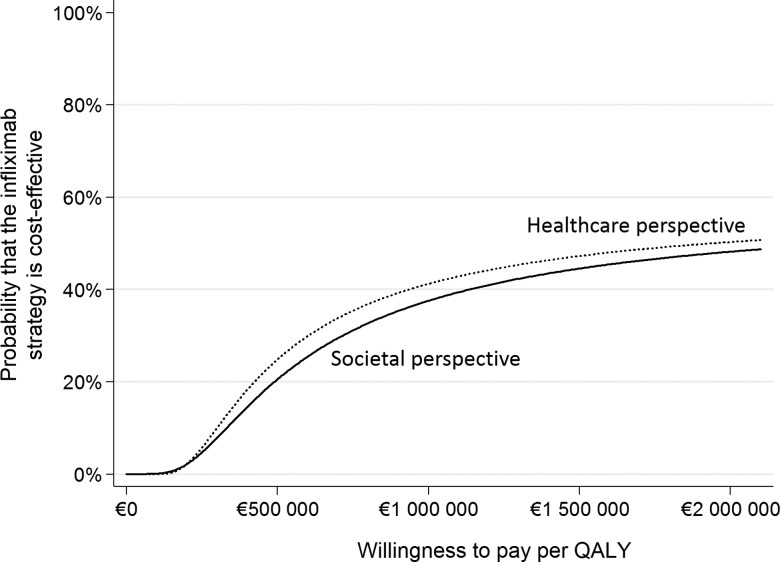
Of 487 patients initially enrolled, 128 and 130 were randomised to infliximab and conventional treatment, respectively. The infliximab group accumulated higher drug and healthcare costs (€27,487 vs €10,364; adjusted mean difference €16,956 (95% CI 14,647 to 19,162)), while productivity losses did not differ (€33,804 vs €29,220; €3961 (95% CI -3986 to 11,850)), resulting in higher societal cost compared to the conventional group (€61,291 vs €39,584; €20,916 (95% CI 12,800 to 28,660)). Mean accumulated quality-adjusted life-years (QALYs) did not differ (1.10 vs 1.12; adjusted mean difference favouring infliximab treatment 0.01 (95% CI -0.07 to 0.08)). The incremental cost-effectiveness ratios for the infliximab versus conventional treatment strategy were €2,404,197/QALY from the societal perspective and €1,948,919/QALY from the healthcare perspective.
In early, methotrexate-refractory rheumatoid arthritis, a treatment strategy commencing with addition of infliximab, as compared to sulfasalazine+hydroxychloroquine, was not cost-effective over 21 months at willingness to pay levels generally considered acceptable.
NCT00764725.
评估英夫利昔单抗与传统联合治疗方案相比,在甲氨蝶呤治疗无效的早期类风湿关节炎患者中进行21个月治疗的增量成本效益。
在这项多中心、双臂、平行、随机、活性对照、开放标签试验中,2002年10月至2005年12月期间从瑞典15家风湿病诊所招募症状持续时间<1年的类风湿关节炎患者。在甲氨蝶呤单药治疗3 - 4个月后,未达到低疾病活动度的患者被随机分配接受英夫利昔单抗或柳氮磺吡啶+羟氯喹(传统治疗组)。药物成本、医疗保健使用情况和生产力损失从全国登记处获取,而欧洲五维健康量表效用值每季度收集一次。
最初纳入的487例患者中,分别有128例和130例被随机分配至英夫利昔单抗组和传统治疗组。英夫利昔单抗组累积的药物和医疗保健成本更高(27,487欧元对10,364欧元;调整后平均差值16,956欧元(95%CI 14,647至19,162)),而生产力损失无差异(33,804欧元对29,220欧元;3961欧元(95%CI -3986至11,850)),与传统治疗组相比,社会成本更高(61,291欧元对39,584欧元;20,916欧元(95%CI 12,800至28,660))。平均累积质量调整生命年(QALYs)无差异(1.10对1.12;调整后平均差值支持英夫利昔单抗治疗0.01(95%CI -0.07至0.08))。从社会角度看,英夫利昔单抗与传统治疗策略的增量成本效益比为2,404,197欧元/QALY,从医疗保健角度看为1,948,919欧元/QALY。
在早期甲氨蝶呤治疗无效的类风湿关节炎中,与柳氮磺吡啶+羟氯喹相比,以添加英夫利昔单抗开始的治疗策略在通常认为可接受的支付意愿水平下,21个月内不具有成本效益。
NCT:00764725 。