Warren Fiona C, Stych Kate, Thorogood Margaret, Sharp Deborah J, Murphy Marie, Turner Katrina M, Holt Tim A, Searle Aidan, Bryant Susan, Huxley Caroline, Taylor Rod S, Campbell John L, Hillsdon Melvyn
Primary Care Research Group, University of Exeter Medical School, St Luke's Campus, Heavitree Road, Exeter EX1 2LU, UK.
Trials. 2014 Apr 21;15:134. doi: 10.1186/1745-6215-15-134.
Interventions promoting physical activity by General Practitioners (GPs) lack a strong evidence base. Recruiting participants to trials in primary care is challenging. We investigated the feasibility of (i) delivering three interventions to promote physical activity in inactive participants and (ii) different methods of participant recruitment and randomised allocation.
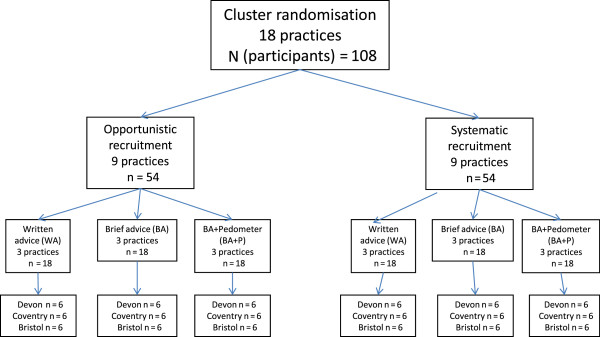
We recruited general practices from Devon, Bristol and Coventry. We used a 2-by-2 factorial design for participant recruitment and randomisation. Recruitment strategies were either opportunistic (approaching patients attending their GP surgery) or systematic (selecting patients from practice lists and approaching them by letter). Randomisation strategies were either individual or by practice cluster. Feasibility outcomes included time taken to recruit the target number of participants within each practice. Participants were randomly allocated to one of three interventions: (i) written advice (control); (ii) brief GP advice (written advice plus GP advice on physical activity), and (iii) brief GP advice plus a pedometer to self-monitor physical activity during the trial. Participants allocated to written advice or brief advice each received a sealed pedometer to record their physical activity, and were instructed not to unseal the pedometer before the scheduled day of data collection. Participant level outcomes were reported descriptively and included the mean number of pedometer steps over a 7-day period, and European Quality of Life (EuroQoL)-5 dimensions (EQ-5D) scores, recorded at 12 weeks' follow-up.
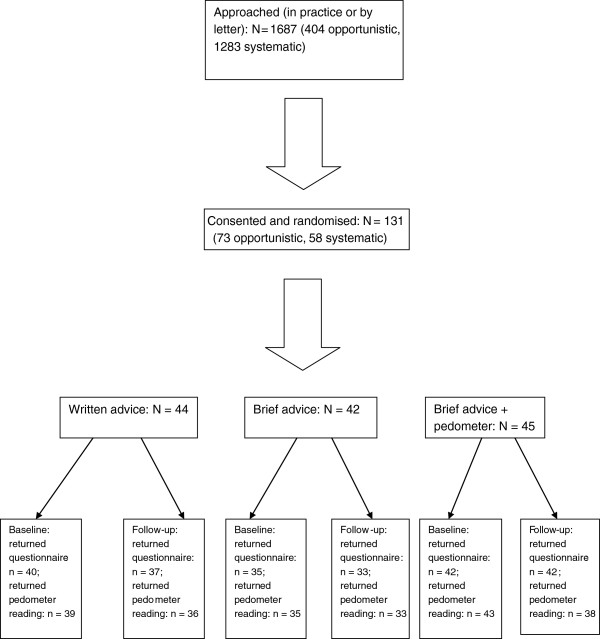
We recruited 24 practices (12 using each recruitment method; 18 randomising by cluster, 6 randomising by individual participant), encompassing 131 participants. Opportunistic recruitment was associated with less time to target recruitment compared with systematic (mean difference (days) -54.9, 95% confidence interval (CI) -103.6; -6.2) but with greater loss to follow up (28.8% versus. 6.9%; mean difference 21.9% (95% CI 9.6%; 34.1%)). There were differences in the socio-demographic characteristics of participants according to recruitment method. There was no clear pattern of change in participant level outcomes from baseline to 12 weeks across the three arms.
Delivering and trialling GP-led interventions to promote physical activity is feasible, but trial design influences time to participant recruitment, participant withdrawal, and possibly, the socio-demographic characteristics of participants.
ISRCTN73725618.
全科医生(GP)促进身体活动的干预措施缺乏有力的证据基础。在初级保健机构招募试验参与者具有挑战性。我们调查了以下两方面的可行性:(i)对缺乏运动的参与者实施三种促进身体活动的干预措施;(ii)采用不同的参与者招募和随机分配方法。
我们从德文郡、布里斯托尔和考文垂招募全科医疗诊所。我们采用2×2析因设计进行参与者招募和随机分组。招募策略要么是机会性的(接触到全科医疗诊所就诊的患者),要么是系统性的(从诊所名单中选择患者并通过信件联系他们)。随机分组策略要么是个体随机,要么是按诊所群组随机。可行性结果包括每个诊所招募到目标数量参与者所需的时间。参与者被随机分配到三种干预措施之一:(i)书面建议(对照组);(ii)全科医生简短建议(书面建议加上全科医生关于身体活动的建议),以及(iii)全科医生简短建议加上一个计步器,以便在试验期间自我监测身体活动。被分配到书面建议或简短建议的参与者每人都收到一个密封的计步器来记录他们的身体活动,并被指示在预定的数据收集日之前不要打开计步器。对参与者层面的结果进行描述性报告,包括7天内计步器步数的平均数,以及在12周随访时记录的欧洲生活质量(EuroQoL)-5维度(EQ-5D)得分。
我们招募了24家诊所(每种招募方法各12家;18家按群组随机分组,6家按个体参与者随机分组),共131名参与者。与系统性招募相比,机会性招募达到目标招募人数所需时间更少(平均差值(天数)-54.9,95%置信区间(CI)-103.6;-6.2),但失访率更高(28.8%对6.9%;平均差值21.9%(95%CI 9.6%;34.1%))。根据招募方法,参与者的社会人口学特征存在差异。在三个组中,从基线到12周,参与者层面的结果没有明显的变化模式。
实施并试验由全科医生主导的促进身体活动的干预措施是可行的,但试验设计会影响参与者招募时间、参与者退出情况,甚至可能影响参与者的社会人口学特征。
ISRCTN73725618。